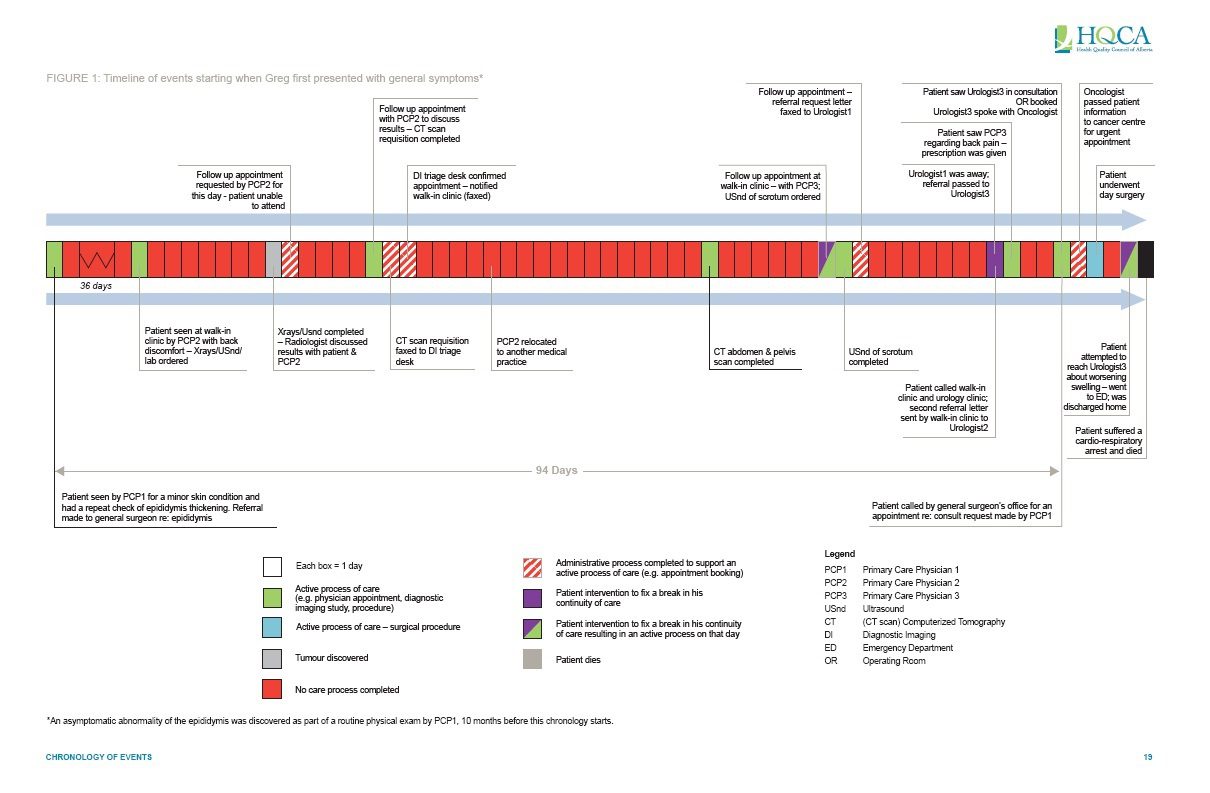
Canadians saw the worst-case scenario of a disjointed health care system in 2012, when Greg Price died after a series of missed communications. One of the key problems was a missed test result. After a doctor at a walk-in clinic found a mass in his abdomen that he worried could be cancer, he ordered an urgent CT scan.
{kind=link}
Three weeks later, that scan was performed — during which time the doctor Greg had seen had left the walk-in clinic. Because of that, the office never called Greg with his CT scan results. It was only after he called the clinic himself that another physician reviewed the test with him, and referred him to a urologist.
“Greg tried to do what he could, but you’re really swimming in the dark on a lot of it, because there’s so much outside the patient’s control and knowledge, to the point where you flounder,” says Dave Price, Greg’s father, who has worked to encourage change in the system since his son’s death. “Patients need to be full partners, able to be part of a decision making process, and fully knowledgeable along all of the steps.”
Greg’s death provoked a Continuity of Patient Care study from The Health Quality Council of Alberta that was released in late 2013, with 17 suggested changes to improve the system. A follow-up report released this summer found that only three of those suggestions have been fully implemented, and 11 are at a high risk of not being done. Among the unfulfilled recommendations is the implementation of electronic systems that would automatically notify pathologists when the doctor that ordered the test had seen the results.
Right now, doctors are often sent test results by fax or through the mail. “We learned from our interviews in this review that radiologists spend a lot of their time trying to track down physicians about critical test results, let alone non-critical test results,” says Eric Wasylenko, medical director of Health System Ethics & Policy for the HQCA. “If they couldn’t get the physician, then they would actually call the patient themselves, perhaps to refer them directly to the emergency department. We want there to be a mechanism that is far more reliable than the current one.”
Another recommendation from the HQCA was to create a personal health portal that would allow patients to see and add to their own health records, including lab results and diagnostic imaging reports. Nova Scotians already have access to this, with a province-wide patient portal for test results that has just been launched; in Ontario and BC, LifeLabs also offers its patients non-crucial results online.
Meanwhile, as part of its regular updates, the College of Physicians and Surgeons of Ontario is also reviewing its Test Management Policy with an eye to continuity of care. “There are some potential vulnerabilities or weaknesses in our system,” says Andrea Foti, manager of the policy department for the College of Physicians and Surgeons of Ontario. “Are there good linkages between specialists and primary care, are there good linkages and flags to follow up on urgent results? And what if an urgent result comes in after hours?”
There are more mismanaged test results more than you might think: An article from The Canadian Medical Protective Association looked at complaint case files from 2006 to 2010, and found that 76 cases were a result of mismanagement of tests and diagnostic imaging reports, mostly involving family physicians, and mostly for failure to properly follow up on tests. A systematic review looked at ambulatory patients in the US and found “significant safety issues” in missed test results. The studies it looked at showed there weren’t documented follow ups in many cases, ranging from 7% to 62% for lab tests, 1% to 11% for abnormal radiology, and 11% to 36% for mammograms.
It’s also telling that 25% of family doctors in Ontario reported they’d had to repeat a test (or procedure) in the past month because the results were unavailable. That number is even higher in some other provinces, rising up to 39% in Manitoba.
“Anytime we don’t get the right [test result] information in the right people’s hands in a timely way, it can become a critical problem,” says Wasylenko. “But it can be solved with the right systems in place.”
The patient side: New websites let patients see their own results
“No news is good news” is becoming a thing of the past, as test results management moves toward websites that allow people to see their own results. New web-based systems are allowing patients the ability to see their test results — sometimes even ahead of their doctor. In the US, the Mayo Clinic, Intermountain Healthcare, the department of Veterans Affairs and Kaiser Permanente all offer patient portals. In Canada, Lifelabs offers access to test results to 1.25 million patients in BC and Ontario. And Nova Scotia recently became the first province to introduce a province-wide system that allows patients to see their test results, called myHealthNS.
“The thinking is that an engaged patient is a healthier patient,” says Chris Faulkner, project manager of myHealthNS. “Literature indicates that patients who have access to their health information take a more active role in their health care.” Some portals in the US automatically also include general guidance on what an abnormal test result might mean.
Nova Scotia’s system allows physicians to control the release of the results, so that they can select some categories to never release automatically, such as HIV results. It also offers the option to put a delay on results so that the doctor can review them first. But myHealthNS recommends to physicians that they automatically release results, because it’s less work. “During our pilot, we had a couple of our physicians who automatically released all results, and they put in their standard message something along the lines of, ‘You may be receiving these results before I’ve had a chance to review them, but I will be reviewing them within the next X days, and if there are any concerns, our office will be in touch to book an appointment,” Faulkner explains.
That’s especially beneficial for patients with chronic conditions, who can use these results to get a sense of their condition over time, says Sue Paish, the CEO of Lifelabs. “What a patient sees is the range around normal — we call those reference ranges — and it shows them where they are on that range,” she explains, adding that they don’t delve into the meaning of abnormal results. “We appreciate that patients need reports that they can understand, but we are also very alert to the importance of the physician-patient relationship, and the physician gives medical advice or guidance. We do not go into that territory.”
Their portal also doesn’t include the results of some tests, including genetic screening and cancer tests. “You will never receive a result that is a serious or critical result by opening your email,” says Paish. “Those kind of results need to be delivered person to person, partially because of the impact of the result, but also because the physician often needs to take action.”
The pilot phase of Nova Scotia’s project, which included 6,000 patients, highlighted other benefits. It reduced waste in the system — Faulkner’s group found that over 60% of patients in the pilot would have called their family physician if they hadn’t had online access to get their test results, and many would book appointments as well, often just to find out that their test results were normal.
A patient portal might also help patients ensure their tests don’t get misplaced – but doctors also “need to try to be cautious that we’re not simply downloading responsibility onto patients,” says Foti. “We want to support patients’ decision making and autonomy, but our job as a regulatory college is to set expectations for doctors to take the positive action they need to take to ensure that care is provided.”
But “a personal health portal meets some really important principles: it finds a way to involve patients appropriately, and helps them manage their own care,” says Wasylenko. “It’s one more way to assure safety.”
The provider side: creating better systems for doctors
One of the key recommendations in the HQCA report was to work towards creating a provincial clinical information system (CIS), which would, among other things, tie together the electronic health record systems throughout the province. But the report suggests that kind of a system is more than 10 years away from implementation. It would allow for a critical test results management system that would flag the 10% of diagnostic imaging results that detect urgent issues and track when those results were reviewed by a physician — what’s known as a closed-loop system.
In that system, doctors would be alerted through an electronic medical record (EMR) system that might have a “critical test result inbox” or through an email to send an automatic receipt that it’s been read. (EMRs aren’t foolproof — doctors can open an alert and not act on the test results. One study found that 11% of critical imaging alerts through EMRs lacked the proper follow up.)
Another thing that isn’t standard — but should be, according to Wasylenko — is a continuously updated provider registry that would have up-to-date contact information for physicians, and offer a colleague to contact instead when a physician is away on vacation. This would also allow an EMR alert to be routed to another physician.
Gaps in test management can also be a problem within hospitals, says Janice Kwan, staff physician in general internal medicine at Mount Sinai Hospital and assistant professor of medicine at the University of Toronto who has written about this issue in the British Medical Journal. “Care transitions in particular are a very vulnerable period in a patient’s journey, where there are multiple handovers, from the emergency department to inpatient care team, or inpatient team to outpatient family physicians and specialists,” she says.
Within the hospital, the process isn’t standardized, she says. An emergency room physician who receives the results of a test they ordered might follow up with the admitting doctor who is now caring for the patient by email or by phone. “The practice is actually quite variable in terms of how individual physicians close the loop,” she says.
But discharge is typically a more formalized process. Hospitals try to encourage closed-loop communication through detailed discharge summaries that are supposed to be reviewed with patients. “Let’s say a critical test result has not been reported yet. We would say to the patient, we expect to receive it in a week’s time. We will contact you with the results, but if you do not hear from us in a week, please reach us at the following number,” she explains. Arranging follow-up appointments after the tests results are expected back is another way to close that loop.
Dave Price is not convinced we’re close to getting where we need to be around test results, or around continuity of care in general. “Whenever we do a public presentation [about Greg’s story], there are always people that come up to us afterwards and say, I had a similar experience, but I was lucky,’” he says.
Yet “pretty consistently the attitude in the system towards our efforts for change has been defensiveness and resistance,” he says, adding that they have “huge respect” for the front-line health care workers. When the HQCA follow up report found minimal progress, he says, “we weren’t surprised.”
“I’m a farmer, and that creates a mindset that there’s a problem, let’s figure out a solution — if you don’t do that as a farmer, you don’t succeed,” he says. “That’s why it’s particularly frustrating looking at a system that is relied upon for people’s lives, where the attitude is ‘it’s not my problem.’”

The comments section is closed.
My family and I are totally confused with my father’s diagnosis. He had colorectal cancer 10 years ago, this was all cleared with chemo and radiation, last year 2019 he had cancer in the sinuses, again he had to get radiation. Then in October he had a TAVI procedure (artificial bovine valve inserted) prior to this procedure he went for a physical, including a blood test. He’s also on blood thinners, cholesterol and water pills. Now they found 2 tumours in his liver… Our question with all these blood test that he has constantly done every 3 months, for the past 3 years as well as the odd ct scan, why hasn’t one of these doctors notice this in the results?
Hi Greg, my name is Donna And I am living in hell because of the health care system, I wish there was something I could do to get help. but I have tried everything that I can think of and there is no help for me. in 2013 I could not take it any longer so I reported the Doctor I was seeing at the time for not doing anything to find out what was wrong with me. and she did nothing. when I reported her for not doing anything to find the problem as to why I was so ill. and they told me she had not done anything wrong. because she would have had to have done something, to have done something wrong. now all Doctors I have seen since are abusing me something tearable. and I have called lawyers everywhere and they tell me there is nothing they can do, the Doctors lawyers are to strong and the doctors cover their asses to much and it is to hard to prove what they are doing. they should not have this much power. I do know that what ever I have is killing me slowing but I am at the end of my rope tring to get help. I need help so bad and I am so ill I do not think I am going to be here much longer, but there is nothing I can do about it. please help me if you can.
Thanks For Sharing
My doctor ordered an urgent can scan, They said the results would be at docs that very day. I called the office and they said doc that ordered was off. I asked them if another doc could speak to me, they said Nope. Another day of worrying and missing work.
If I cant see some test results does that mean something is wrong ?
Only testing to the lowest measure can also leave out a lot of information. The physician should have a responsibility to check the results and also retest if there is any doubt. Many persons healthy can normal falls slightly outside the measures of clinical norms. A doctor can know if there patient is becoming unwell by seeing whole results. For example someone with very low blood sugar historically then their sugar sits at the high range of normal, may be becoming critically ill. Simply looking if it fell in the laboratory’s marker for normal or not will not render a physician the full medical patterns and therefore treatment. Patients checking there own results is not always a good idea especially anyone with mental illness or limited medical skills may misinterpret or forget to check, ask someone else who is not authorized to check which goes again PHIPA, and also it certainly leaves the door open to hackers, and much misunderstanding about results even in someone who is highly educated.
I have just discovered that my blood tests show a very high colesterol and very high LDL. My colesterol levels have always been hig but my HDL was always higher than LDL. I have discovered there are many reasons that can cause this. I believe they made a mistake. I don’t eat red meat I eat a lot of foods and fish oil supplaments. I don’t eat sweets with a lot of sugar and very little salt and I rarely eat processed foods. I do take prescription pills for high blood pressure that could cause this and I refuse to take stattons. Why don’t doctors know that ssome drugs cause false high colesterol readings.
The evidence for improved outcomes when patients are linked to one health are provider team (often called ‘medical homes’ is apparently clear. However, care and support that enables us as individuals and families to be healthy, stay healthy and achieve our ‘life goals’ is in reality a multifaceted set of relationships, services etc. If our ‘health support system’ is truly patient centred.. could we consider a ‘health home’ that is in fact, more virtual than ‘touchable’; our ‘medical home’ or family doctors office would be a critical part, but in this information age, would a ‘virtual ‘home base’ that includes all information and communication that is relevant to ‘me’ be collected in one place, including all the resources and contacts that I as an individual. If this ‘virtual health home’ was accessible to me and to any provider that I chose to give it to.. wouldn’t this enable continuity of care regardless of where I am. Of course in Canada, these ‘virtual health homes’ would need to be provincially based, but if I could access (and give access) from anywhere, I can see the benefits.
Interesting article. However, I don’t see how online portals that don’t send all results to patients will solve the issue of crucial results being ignored by docs. If they aren’t also shared with the patient there is no change in the likelihood that somethings will be lost to follow up. As well, life labs in BC shares results with patients only if they have a BCMSP number, about a third of my patients are from other provinces so they cannot use the eHealth service. Patient portals that originate from the practices EMR would be more reliable.
Yes.
Patient portals are contingent upon the patient/caregiver then having an efficient and relatively barrier free (I.e. Not being put on hold for 20 min or a Byzantine set of CYA verbiage and “press 1 for”, “press 2 for” only to be followed by being shunted somewhere else) method of communicating this back to the clinician and then communicating with the clinician about it – both of which are sorely lacking in general (although pockets of excellence exist). Without this, this is just a recipe for needless worry and unnecessary trips to urgent care and EDs.
(the private industry trend – some telecoms, banks, etc – of telling approximate time to speak to the clinician followed by a call-back rather than waiting on hold would be a good, but insufficient, start.)
I think bringing the patients into the picture is great, but access to the data is only part of the problem.
Without the links back to the provider of continuity, the evitable result is the involvement of other providers based on availability and then unnecessary and/or redundant testing.
I wonder if the system in BC (and elsewhere) started by asking… how will the patient get all of their information in a timely fashion (regardless of province of origin) whether the decision would have been different? By extension, the patient hopefully could share that information with whatever provider was involved.
From experience as a caregiver for 15 years, I can attest to this being more than an occasional problem. As Trevor Jamieson points out, it shouldn’t require rocket science to resolve.
Dave Price’s comments (at the end of the article) are indicative of a much greater barrier – one that impedes improvements in many aspects of healthcare, i.e. a consistent attitude of defensiveness and resistance to change. Matthew Syed, in his book “Black Box Thinking – The Surprising Truth About Success (and Why Some People Never Learn from their Mistakes)”, provides numerous insights into why this is so, not least that it is a natural human reaction not to admit to mistakes or omissions (even to ourselves). Applied at the organisational level it is, however, a formula for failure: again as Mr. Price indicates, we can only improve our own and organisations’ performance by recognizing errors and omissions, investigating systemic causes of them and devising solutions to prevent their re-occurrence. This approach to doing business in the air transportation industry has resulted in a truly staggering safety record.
There are clearly “centres of excellence” in our healthcare system but all too often, even at the highest levels, “we” seem to do the exact opposite of this: the examples are legion but two of the most egregious are; the painfully frequent assertions that we have one of the best healthcare systems in the World when research done by the World Health Organisation, the OECD, the Commonwealth Fund and the Euro-Canada Health Consumer Index demonstrate that is patently untrue; and the attempts (by practically all provinces) to impede the CBC in producing the programme “Rate Your Hospital” a couple of years ago.
Only the real commitment of senior management within the healthcare system can change the “culture” of “defensiveness and resistance” to one of transparency, disclosure and learning from errors and omissions. (Mathew Syed’s book would be a good place to start – since its publication he was engaged as an adviser to the UK National Health System.)
Frankly, some of these issues don’t need multi-million dollar fixes and we often overthink the first steps.
Step 1 – stop trying to call me or fax me with this stuff – please. I’m too busy to take calls, and faxing is inefficient (both for information transfer and trees) and faux-secure – I don’t walk around with a fax machine on my person, and I never will. I’m connected to email and texting all the time. Sure, all versions aren’t necessarily secure, but, I was using secure versions of both of these in the IT world in the early 2000s. Email, in particular, is a 30 year-old technology (in the public sphere – the first emails were actually sent back in the 70s) that we are still trying to formulate an opinion on in much of health. It’s kind of nuts.
While security is batted around as a major issue, like I said, secure versions of peer to peer communication have existed forever, and don’t need to break the bank.
The bigger issue is mentioned in the article: identity.
While many physicians lack a secure electronic contact, those that do aren’t necessarily easier to contact. Many have multiple addresses (with restrictions on forwarding from one account to another) and many people have name reconciliation issues because they have the same name as someone else or because their contact name doesn’t match their professional name (nicknames, maiden names, etc). This is also not a difficult fix: index the electronic contact to a unique key – CPSO # seems natural for physicians – and allow people to have one primary clinical address that the others can be forwarded to (or even better – stop giving me different email addresses and allow me to have one @doctor.on.ca or @ontariomd or whatever is decided).
That me emailing myself at another institution is potentially considered a privacy breach is asinine. Importantly, as more and more newer MDs spread their work across multiple practices, the exact same issue of sending things to the “right” fax machine exists – but we sweep that one under the rug and generally ignore it allowing people to have one and only one fax number for information – while if you suggest that I might get an email or secure text at one hospital for a patient I saw at another, suddenly the sky is falling.
Another issue is raised and is very legit – coverage. When people are away, have locums, etc, you don’t want communication going into the ether. (Importantly, this is even worse for faxing as, whether away or not, I’m going to periodically get emails/texts and can direct the sender to the right person). Again, this doesn’t need to be a trillion dollar fix – a system that allows assigned coverage and message forwarding is not that novel. In health care we treat these things as if they are patentable revolutions.
Start with the easy wins. The security already exists. The policies needs revamping.
When I did blood tests and imaging in my practice, I always told patients that with me, no news meant there had been a breakdown in the communication chain. It could be at the testing institution, their report to me, my staff not getting it to me, my misfiling it, my getting the information back to my staff and my staff getting back to the patient. So there are lots of places for the chain to break. I told each patient that if they had not heard from my office by a specific time, which depended on the urgency of the situation, that they should call my office. Some doctors have patients make appointments to discuss the results to ensure that the patients’ results have not been lost in the shuffle. For someone like me, who only ordered a few tests per week, that was not too onerous. I feel for family physicians who must look so many test and imaging results and then communicate them to their patients.
With the large demands on physician time and the busy lives of patients in 2016, this is a big problem. I hope that a workable and safe solution can be found.