Despite warnings from international health authorities that COVID-19 can be spread through aerosol transmission, our public health agency has yet to alert Canadians.
The Public Health Agency of Canada (PHAC) maintains that COVID-19 is spread by the three Cs – close contact, contaminated surfaces and common greetings – that has resulted in the ubiquitous advice to stay two metres apart from one another, wash our hands frequently and wear masks.
However, a recent outbreak in an indoor spin studio in Hamilton indicates that updating this guidance is increasingly important as we move indoors amidst a second pandemic wave. Despite apparently following public health directives and cutting its classes in half to allow a six-foot radius for all bikes, at least 72 cases have been attributed to the class.
“This is not about how well the gym was run; this is about how COVID spreads,” Colin Furness, an infection control epidemiologist at the University of Toronto, told The Hamilton Spectator. “If you let people hangout together, without masks, sharing air, in the same space for a prolonged period of time … this was going to happen anyways.”
When people cough, sneeze, talk, exercise or sing, droplets in a range of sizes are expelled from their mouths and noses; the smallest are called aerosols. Larger droplets within two meters of the infected person are the primary way the virus spreads. But there has been controversy over those smaller droplets, the aerosols.
In July, hundreds of experts signed an open letter to the World Health Organization (WHO) that successfully petitioned for it to acknowledge aerosol transmission of COVID-19. The United States’ Centres for Disease Control and Prevention (CDC), after first succumbing to political pressure, acknowledged on Oct. 5 that “there is evidence that under certain conditions, people with COVID-19 seem to have infected others who were more than six feet away. These transmissions occurred within enclosed spaces that had inadequate ventilation.”
In Canada, however, PHAC has said “The understanding of aerosol transmission of COVID-19 continues to evolve,” and has not recognized that the virus can spread through aerosols. In a statement on Oct. 9, it noted: “Aerosol transmission refers to when the very small droplets containing the virus that are released when an infected person coughs, speaks, talks, shouts or sings are suspended in the air for a period of time and breathed in by another person. How often this occurs, and under what conditions, is not well understood.” The agency says it will update its guidance in coordination with other agencies to avoid public confusion.
Dr. Nelson Lee, an infectious disease physician in Edmonton, says the definition of “airborne transmission” is causing confusion. “When we talk about aerosol transmission, it is not the explosive type of transmission, like measles or tuberculosis, where you can actually smell the virus and get it through the air. It’s not like that. We are trying to point out that there’s a significant potential of these microdroplets, or aerosols, spreading beyond two metres.”
Lidia Morawska of the WHO Collaborating Centre for Air Quality and Health in Brisbane, Australia, leads an international effort to build evidence and draw attention to the risk of COVID-19 spreading through aerosols. She recommends that building managers keep their heating, ventilation and air-conditioning (HVAC) systems well maintained to limit or reduce the amount of recirculated air.
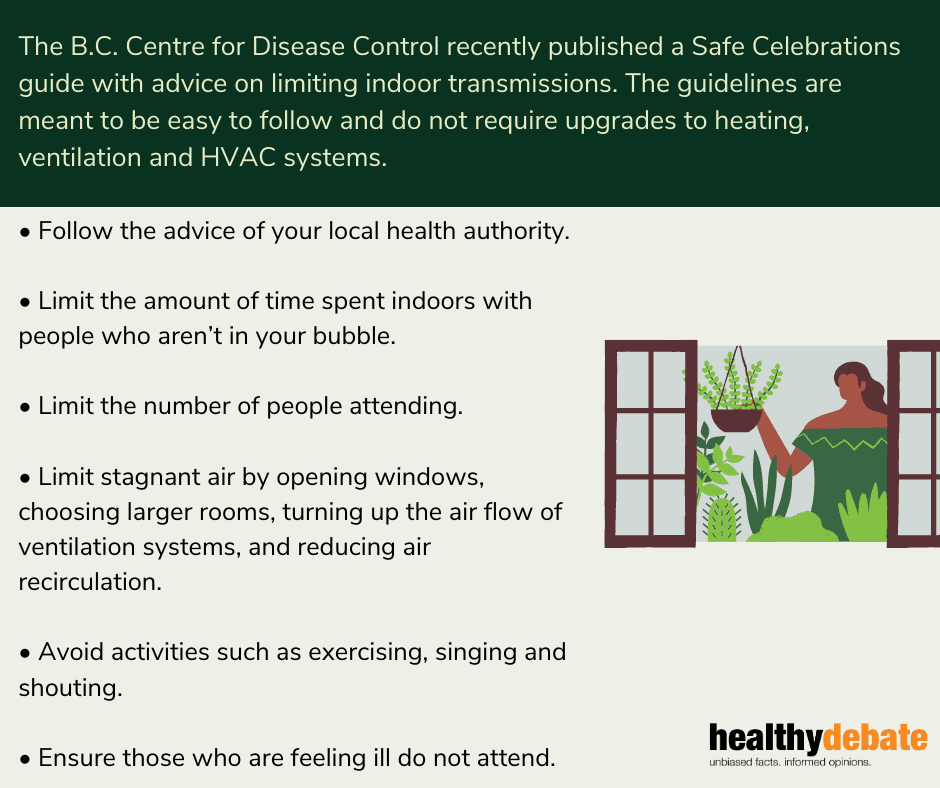
Morawska notes that as people head indoors for winter and look forward to seasonal celebrations, proper ventilation will be important as it can provide an additional layer of safety.
Jeffrey Siegel, a professor of civil engineering at the University of Toronto and a member of its Building Engineering Research Group, has been studying the impact of indoor air quality on human health for more than 10 years. “I’ve had more interest in my work on indoor air quality in the past few months than I have had throughout the rest of my career,” he says.
Our indoor public spaces have varying air qualities serviced by different HVAC systems, says Segal, some of which are excellent, some poor and “some of those HVAC systems are archaic.”
The risk is not equal throughout Canada. Several provinces have announced funding to address aging HVAC systems in their schools but there is concern over the amount of time needed for upgrades and the funding involved. Many First Nations, Metis and Inuit communities have long been plagued with poor indoor air quality from overcrowding and housing shortages and are also more likely to have limited access to healthcare services, leaving them vulnerable to the impacts of COVID-19.
In a statement Oct. 9, Indigenous Services Canada said: “In the last few weeks, Indigenous communities have been facing an alarming rise in the number of new and active COVID-19 cases.” It has committed to providing additional rapid COVID-19 testing units to point-of-care testing in First Nations communities, and prioritizing those in rural, remote and isolated communities.
“Our first dollar should be spent on improving the environment of the most disadvantaged individuals,” says Siegel.

The comments section is closed.
Great article Paleah.
I appreciate your last points about Indigenous and rural communities’ air quality and how some communities are affected differently.
We used to hear of aerosols in TV commercial talking about clean air and an aerosol cleaner ie a fabric cleaner or an airspray. I just heard TTC uses one to cleanse buses and it works several hours to protect surfaces people are using. With this info are they’re not air cleansers to purchase like the TTC where people are forced to gather ie waiting lines. In some ways this info is not new. Where are your recommendations to clear the air so to speak, no pun intended.
Thank you Paleah . This is very well researched and written!! It is important to share this information with the public . Well done!
Dr. Tam has referred to public health as a team event which has let to tragic delays and confusion. She and her deputy owe their allegiance to and take their direction from the 12,000 member private organization, the IDSA. Canada agreed to support and follow the lead of the highly conflicted CDC which is now:
1.) “Dying in a Leadership Vacuum”, The editors, NEJM 383:1479-1480; 20-10-08: DOI: 10.1056/NEJMe2029812 https://www.nejm.org/doi/10.1056/NEJMe2029812
Related articles by Prof. Amir Attaran:
2.) Deciding Who Gets Tested Differs across Canada, Causing ‘Chaos and Errors’, Nikiforuk A, The Tyee.ca 20-04-13: https://thetyee.ca/News/2020/04/13/Testing-Across-Canada/
3.) How Canada has bungled the COVID-19 endgame, Attaran A, MacLean’s 20-05-31: https://www.macleans.ca/society/health/how-canada-has-bungled-the-covid-19-endgame/
4.) Canadian leaders botched mandatory masking. Here’s how to fix it, Attaran A, Maclean’s 20-07-15: https://www.macleans.ca/opinion/canadian-leaders-botched-mandatory-masking-heres-how-to-fix-it/
It’s time medicine got back to its scientific roots and away from dogma and Canada developed and followed its own policies.