While economic uncertainty amidst yo-yoing threats from the United States overshadows all other issues in the coming election, Canadian health-care leaders will be listening closely to what our federal politicians have to say on the campaign trail.
Just a matter of months ago, Conservative leader Pierre Poilievre was all but guaranteed a victory. However, recent polling shows the margin between the Conservatives and new Liberal leader Mark Carney is closing. As it stands, it’s anyone’s race.
With Canadians still struggling through a particularly debilitating respiratory virus season, health care is top of mind for many. COVID-19 is still a lethal and disabling force world-wide and other infectious disease outbreaks – measles, mpox, norovirus and avian flu to name a few – all continue to make headlines.
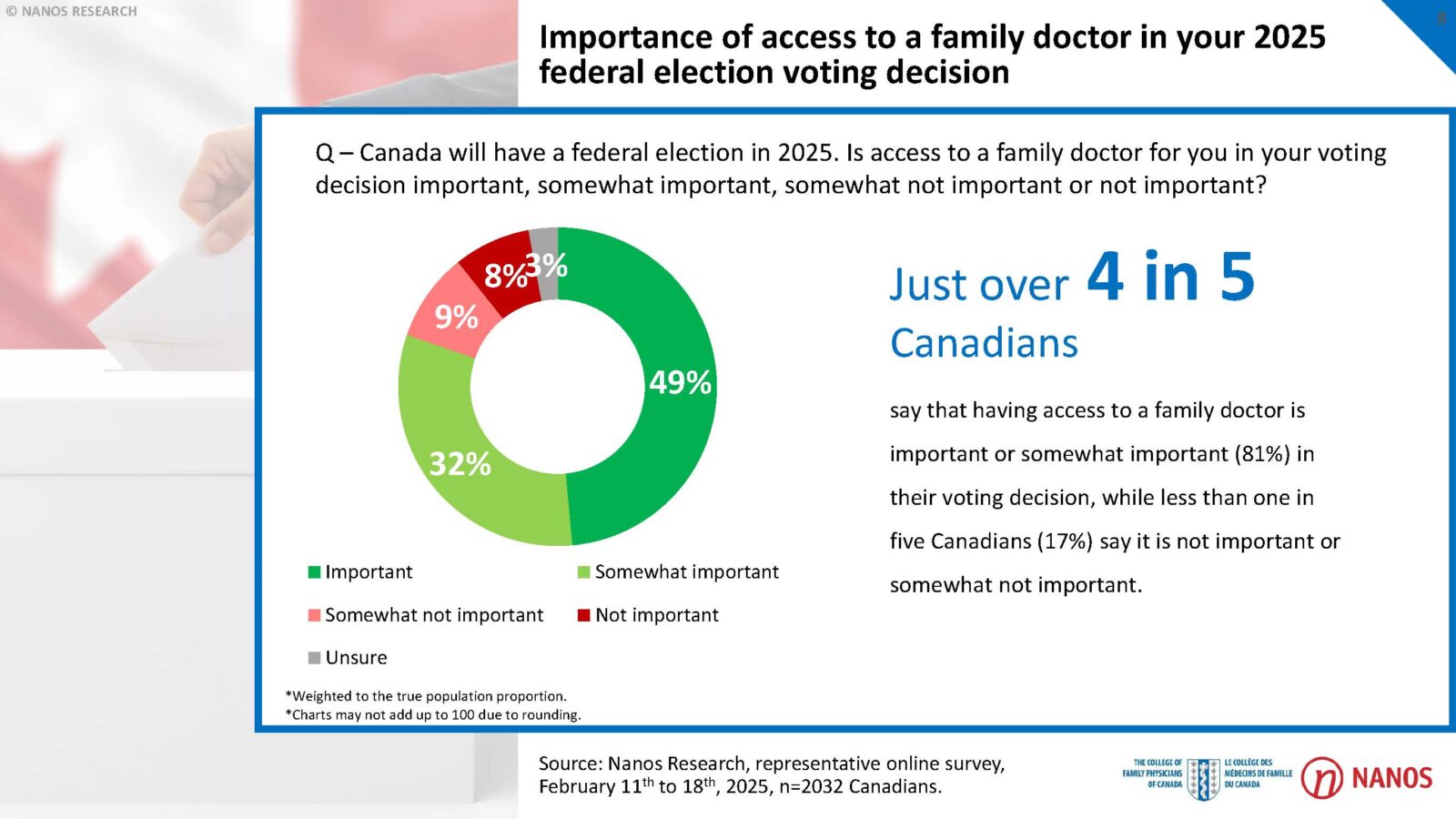
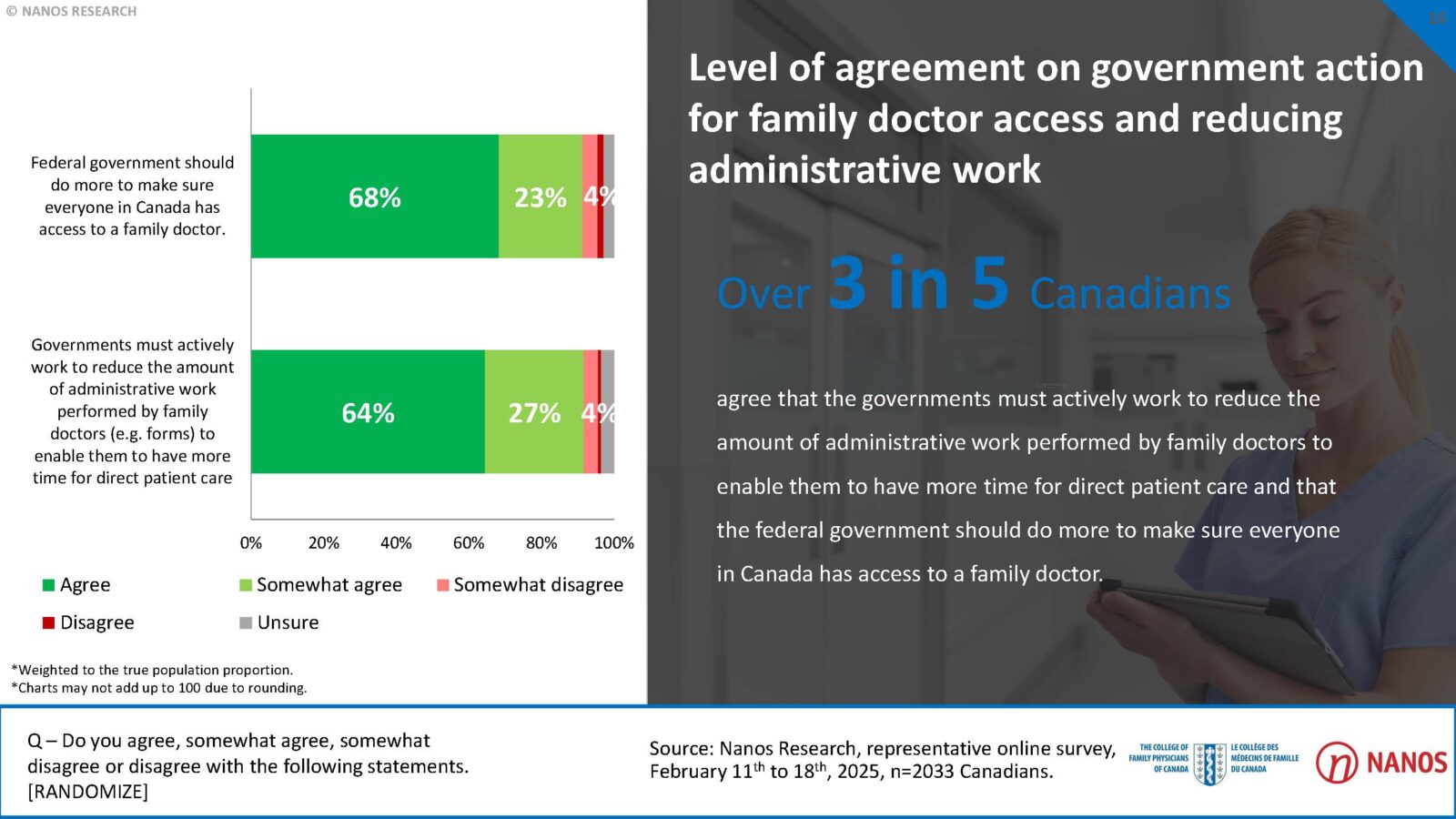
A recent report by Nanos and the College of Family Physicians of Canada indicated that more than 90 per cent say the government should do more to make sure everyone in the country has access to a family doctor.
So, what do health-care experts hope to hear from candidates this election?

The comments section is closed.