Alberta’s emergency departments (ED) are buckling under the weight of 12-hour wait times and catastrophic Emergency Medical Services (EMS) offload delays; a crisis that recently prompted emergency physicians in the province to sound the alarm on unsafe conditions.
Patients in our urban centres, particularly Edmonton, often must endure agonizing waits for minor, easily treatable complaints like a child with a midnight fever, an ear infection or a minor laceration.
The paradox is glaring. During business hours, that same patient would be seen within an hour at a local walk-in clinic or medicentre. However, illnesses and minor traumas do not respect the traditional 9-to-5 workday.
Due to the lack of a robust, after-hours “middle ground” of care, all patients are funneled into Level 1 trauma centres, creating a catastrophic bottleneck. The downstream effects are severe, most notably the trapping of EMS crews in hallway offload delays, effectively stripping our communities of critical 911 response capacity.
Furthermore, these profound delays create severe psychological distress and anxiety for vulnerable populations, particularly children and the elderly, who are forced to labour in crowded, high-stress waiting rooms for hours on end.
Combining frontline clinical medical practice, deep expertise in large-scale operational logistics and specialized insight into the psychological impacts of delayed care, we have observed that the friction in our urban EDs is myriad. Much of it stems from the heavy administrative burdens placed on acute-care hospital nursing staff; barriers that are largely non-existent in the leaner operations of clinics.
We do not need endless government studies to solve this, nor do we need to spend billions expanding the physical footprint of our city hospitals. We need to bridge the gap between acute and non-acute care with a model that is agile, rapidly deployable and economically viable for physicians.
The solution lies in a hybrid partnership model that utilizes mobile infrastructure and the incentivizing of family physicians to decompress the ED from the parking lot.
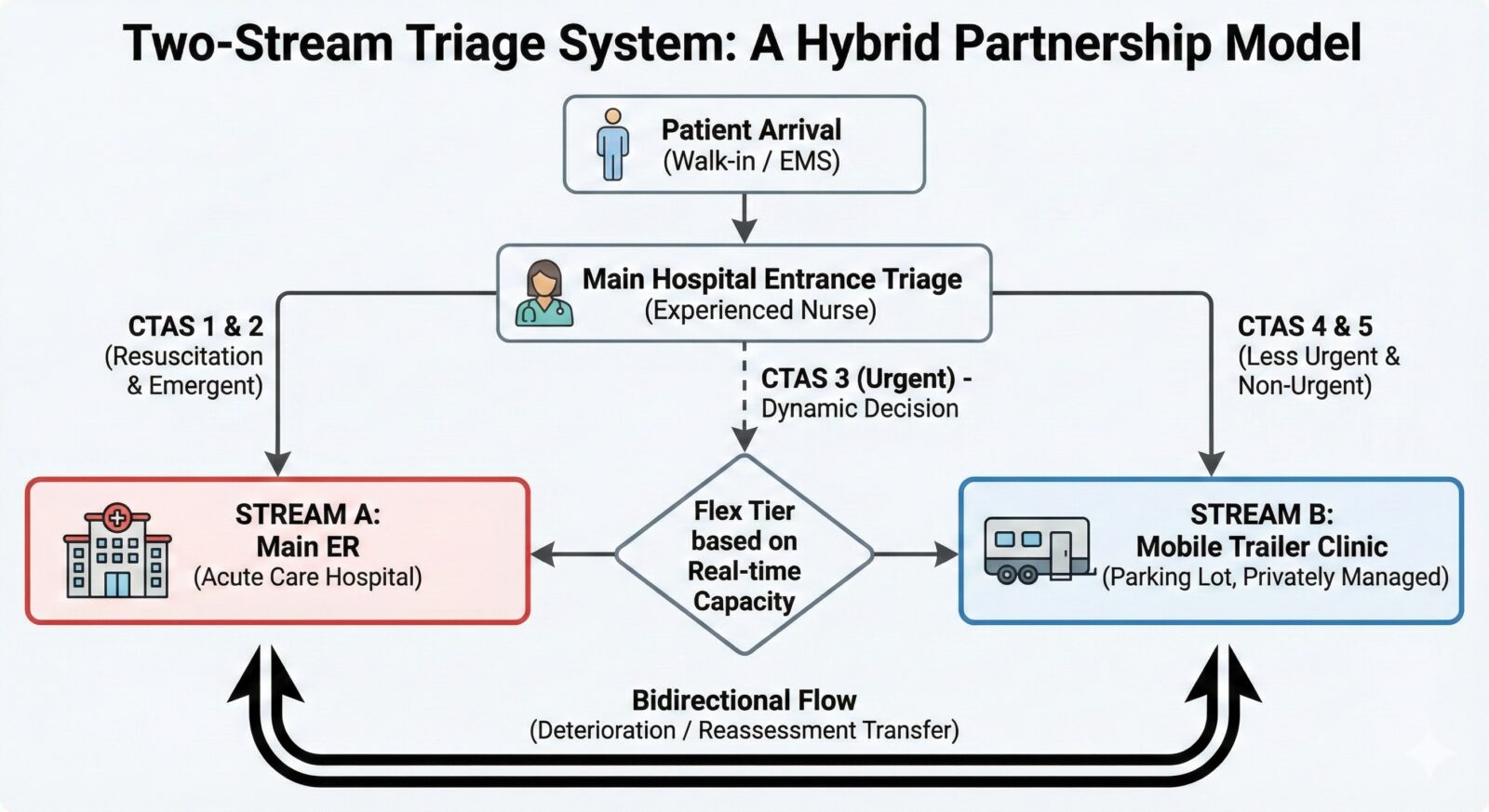 The two-stream triage system (Fig. 1)
The two-stream triage system (Fig. 1)
The core of this model relies on redirecting low-acuity flow before it ever enters the main ED waiting room. Triage would remain precisely as it is today; conducted by experienced triage nurses at the hospital entrance. From there, patients are divided into two distinct streams:
- Stream A (The main ED): Patients classified as CTAS 1 and 2 (Resuscitation and Emergent) are directed immediately into the traditional ED.
- Stream B (The mobile clinic): Patients classified as CTAS 4 and 5 (Less Urgent and Non-Urgent) are diverted to a fully equipped, modular mobile clinic situated directly in the hospital parking lot.
- The flex tier: CTAS 3 (Urgent) patients act as the system’s dynamic pressure valve, directed to either Stream A or Stream B depending strictly on the real-time capacity and wait times of the main ED.
Crucially, this is a bidirectional system. If a patient in Stream B rapidly deteriorates, or if a patient in Stream A is reassessed and downgraded in acuity, they can be seamlessly transferred between the two environments.
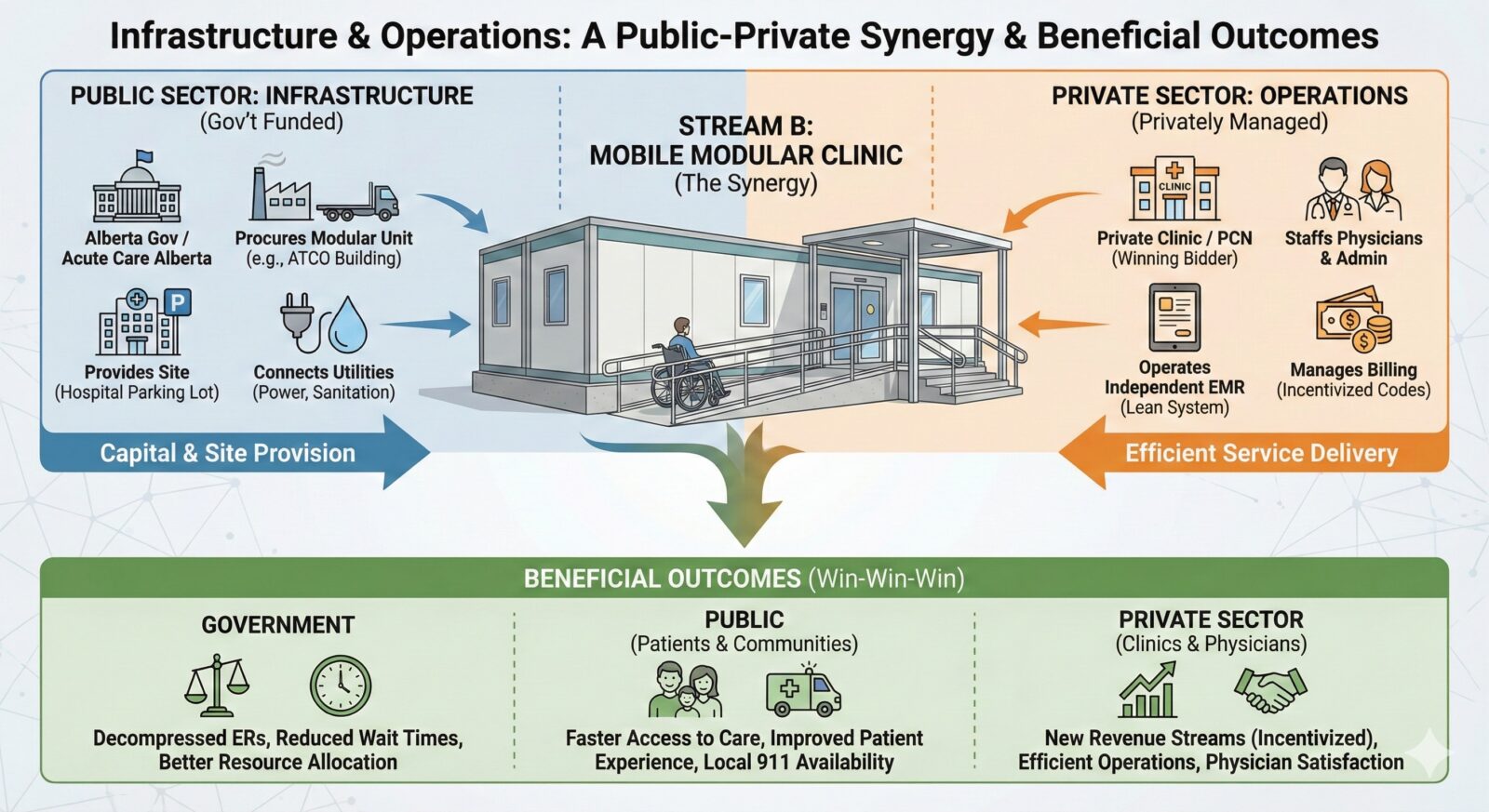 Infrastructure and operations: A public-private synergy (Fig. 2)
Infrastructure and operations: A public-private synergy (Fig. 2)
This model requires zero new permanent construction, utilizing a smart division of labour between the provincial government and private medical enterprise where health services are still covered by the government. The model brings private sector fiscal efficiency to interface with public doors without negatively impacting the responsibilities of the latter; the symbiotic interface is where the goals are achieved.
- The infrastructure (publicly funded):
The physical space should not be a capital burden on physicians. The Ministry of Health, acting through Acute Care Alberta, would procure and provide the physical infrastructure using modular, winterized medical units, such as the health care-specific trailers manufactured locally in Alberta by companies like ATCO. These modular units are designed specifically for clinical use, deployable within weeks and would be stationed directly in the hospital parking lots with dedicated power and sanitation hookups.
- The operations (privately managed):
While the government provides the structure, the operations are entirely outsourced to the private sector to ensure maximum efficiency and minimal bureaucratic bloat. The government would issue a Request for Proposals (RFP) for the management of these Stream B trailers.
- Bidding: Local Primary Care Networks that are collaborative partnerships between local family physicians and AHS, established private clinic conglomerates or newly formed physician co-ops would bid for the operational contracts.
- Management: The winning bidder operates the trailer as a satellite business unit. They are responsible for staffing the physician shifts, providing the clinic manager or administrative assistant, and maintaining a localized, rapid-charting Electronic Medical Record (EMR) system independent of the hospital’s heavier digital infrastructure.
- Billing: The clinic manages its own billing using the incentivized, after-hours Stream B consultation codes, paying the moonlighting physicians directly and keeping a standard overhead percentage to run the unit.
This model essentially takes the highly efficient, high-volume operational machinery of a private walk-in clinic and drops it exactly where the need is most critical. This is at the hospital doors.
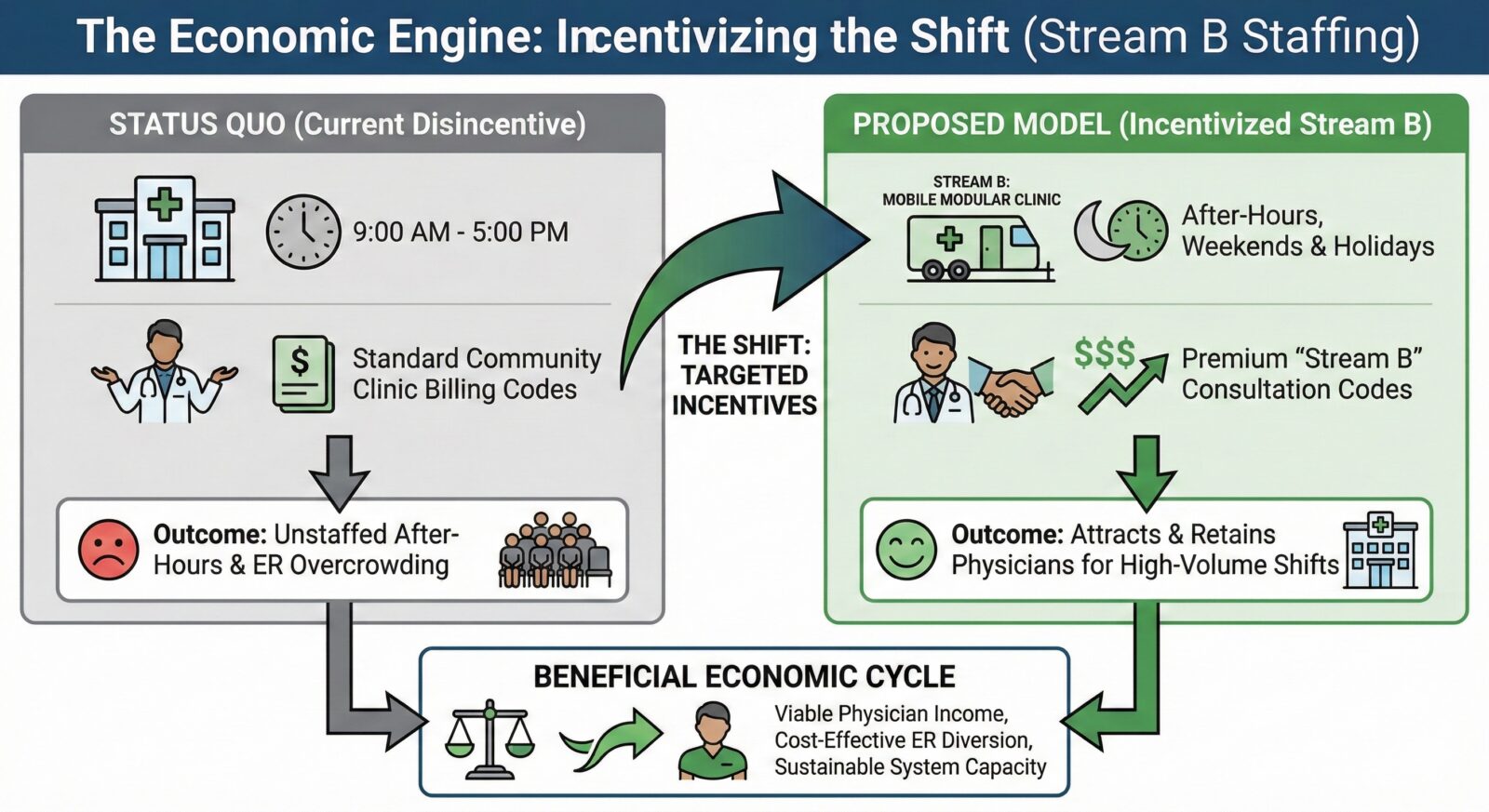
The economic engine: Incentivizing the shift (Fig. 3)
A model is only as successful as its ability to attract and retain physicians. Family doctors already possess the skills to manage CTAS 4 and 5 complaints; what they lack is the framework and financial incentive to do so after hours at a hospital site.
To staff these mobile units, we must implement a targeted billing structure. Physicians working in the Stream B mobile clinic would utilize special consultation codes that pay a premium of 20 per cent to 50 per cent higher than regular community clinic codes, scaled dynamically depending on the time of day or night and statutory holidays.
This mirrors the shift-based and time-of-day incentives already successfully utilized to maintain staffing in rural Alberta hospitals. By adequately compensating family physicians for moonlighting in these high-volume, low-acuity triage units, we create a willing workforce ready to clear the backlog.
We have straw-polled a few urban Family Physicians who all attest that they will be willing to do this work if the incentives are right.
 Proof of concept: A one-year targeted pilot (Fig. 4)
Proof of concept: A one-year targeted pilot (Fig. 4)
We do not need to overhaul the entire provincial system overnight to see if this works. We need a targeted, data-driven, one-year pilot program.
To properly stress-test the model, the province should deploy mobile Stream B units to a maximum of four strategic locations:
- Edmonton: One or two units stationed at major, chronically bottlenecked sites.
- Calgary: One or two units at comparable high-volume sites.
- Regional hubs: One unit in a busy, mid-sized urban centre like Red Deer, which frequently faces severe rural-to-urban diversion pressures.
Over 12 months, we can track exactly how many CTAS 4 and 5 patients are diverted, the reduction in overall ER wait times, the decrease in EMS offload delays and the cost-to-benefit ratio of the physician billing incentives versus the exorbitant cost of unnecessary acute-care hospital admissions.
We cannot continue to treat pediatric earaches with the same heavy, expensive administrative machinery designed to treat multi-trauma car accidents. By establishing contracted, mobile urgent-care trailers in our hospital parking lots, we can bypass the institutional bottlenecks of the main ED, free up acute-care beds, get our paramedics back on the road and finally provide Albertans with the timely, middle-ground care they deserve.

This is a brilliant well thought and structured analysis of our heath system with cost effective solutions. It deserves presentation to the decision makers at both federal and provincial level. It’s tested and working in other health systems abroad, I don’t see why it wouldn’t work in Canada. Thank you for thinking outside the box.
Wow, this article was quite insightful. Thank you for illuminating this issue.
Wow Helen, this is such an important piece of work.
What struck me reading the article is how practical the solution is, no new buildings, no billion-dollar budgets, just a smarter use of what already exists. The two-stream triage model makes so much sense, and the idea of mobile units in hospital parking lots to handle low-acuity cases is exactly the kind of thinking that closes the gap between policy and real people’s experiences.
The way you and your collaborators have brought together clinical, operational, and psychological expertise in one proposal shows what is possible when the right minds work together on the right problems.
Proud to see you, as my mentor represented in a conversation that matters this much. Well done to you and the whole team.
I think this is a prime example of heads coming together to WORK together and come up with a VIABLE solution to a problem that is getting worse exponentially -without spending millions of dollars on Logic.
I believe this program could not only shorten wait times, but it would 100% save lives. Our vulnerable sector needs special attention, as do true emergencies. Too many times in the past, my family’s much needed ER visits were sorted behind people already waiting, that most certainly didn’t look/act/talk like they needed to be there (that may be presumptuous, but it’s definitely an opinion based on what I not only see, but hear currently).
The ER is NOT a Dr’s office substitute for when clinics are closed for the day.
Along with this solution, more advertising for the 811 phone number should be a focus as well. Not only is 811 able to help, but when they can’t they will direct you to a Dr’s office the next day, or to an ER. When I had my first son, the nurses at 811 became my surrogate mother. The IMMENSE support I received from these women honestly helped me become a better Mom. I’ll always be so grateful for them.
I think this is a fantastic solution to ER wait times and crowding. I support common sense and logic. I hope to see this implemented as soon as possible. The health and safety of Albertans is not something that should be delayed any longer. Work in tandem with Dr’s and Administrators that WANT this system to work because they care about patients, and because Dr’s want to continue to make a difference. Lives depend on it- and you don’t need a survey to tell you that.
Finally a solution that makes actual sense!