Michael’s Story
Michael is a 35 year old with a past history of gallstones. He began to feel a stabbing pain in his belly one evening and tried to sleep it off. He was woken up by an excruciating pain, something he’d never felt before, and his wife drove him to the local emergency department.
First, Michael waited in the emergency department to see a doctor, who suspected gallbladder inflammation related to gallstones. The doctor ordered diagnostic tests to confirm this and called for a surgical consultation. The surgeon on-call was busy with a full slate of scheduled cancer surgeries that day, and not wanting to cancel those patients, waited until he had a moment towards the end of the day to see Michael.
By the time the surgeon saw Michael, he realized he needed surgery to remove his gallbladder within the next day. The doctor bumped a patient scheduled for surgery for the next morning and fit Michael in.
Michael is a fictitious patient. However patients like him arrive daily to Canada’s emergency departments. A 2007 Canadian Institute of Health Information report found that about 20% of the one million Canadians admitted to hospital from the emergency department require surgical care, some of it urgent.
An ignored and fragmented patient population
There are many conditions that require urgent surgery, but disorders such as hip fracture, acute cholecystitis (acute gall bladder inflammation) and appendicitis are particularly common.
Time is of the essence in treating patients who require urgent surgery. Delaying an urgent surgery for lengthy periods of time, in some cases, increases complications and may even lead to death. For example, an inflamed appendix, untreated, may rupture, spreading infection throughout the abdominal cavity.
There is a growing body of research suggesting that patients with urgent surgical needs are waiting too long for surgery. From the time that they present to an emergency department to being booked in for surgery, they can experience many periods of prolonged waits.
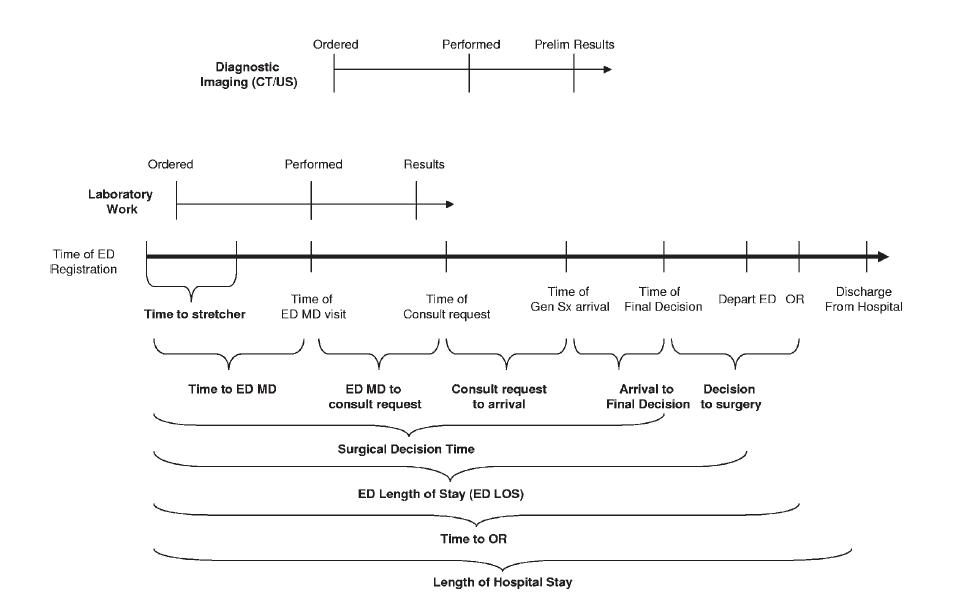
The diagram below, from a study led by surgeons at Sunnybrook Health Sciences Centre in Toronto, shows the many different steps in the typical journey of an urgent surgical patient. It details the waiting periods from the emergency department waiting room to operating room. (Click on the image for an enlarged view.)
Patients with urgent surgical needs are described by the Canadian Association of General Surgeons as a “sometimes ignored and fragmented patient population”. These patients cross many different clinical areas and hospital spaces, in comparison to patients booked into elective surgery.
Surgical services in larger hospitals are often organized by specialty, with operating rooms dedicated towards specific areas, such as cancer and orthopaedics. These are generally scheduled surgeries, with patients having a pre-surgery consult and care.
Urgent surgeries have traditionally been slotted into the existing surgical schedule, wherever they might fit, which can include after hours or else bumping an existing surgery booking. Typically each surgical division and surgeon will be allotted a certain ‘block’ of operating time for their elective surgery. Surgeons use this time to manage patients requiring surgery who have been referred to them. If their ‘elective time’ is continually utilized by ‘urgent surgery cases’, their elective wait lists will grow, ultimately affecting the timeliness and quality of their services.
As there has been increasing attention focused on improving elective surgery wait-times, hospitals and surgeons tend to fiercely protect ‘elective surgical blocks’. In some cases, this may result in urgent cases being delayed until later in the day, when surgeons have completed their elective list of surgeries for the day.
Urgent surgery wait times are not being measured
Measuring surgical wait times is well established across Canada. In 2004, provinces agreed to a 10-Year Plan to Strengthen Health Care, with a major focus on wait times. This plan identified five priority areas for wait time reductions, elective surgeries in cancer care, cardiac care, diagnostic imaging, hip and knee joint replacement and cataract surgery.
The plan set benchmarks for wait times in these areas, and involved a substantial amount of new funding – $1.7 billion in Ontario – to increase the number of these procedures, and a commitment to publicly measure and report on wait times. In Ontario, publicly reporting on wait times for surgery has expanded beyond the five priority areas to a broad range of elective surgery and diagnostic procedures. However, conspicuously omitted from this list are urgent surgeries, such as the one required by Michael.
There are gaps in our knowledge about how long patients are waiting across Canada for urgent surgery. “We’ve made an assumption that patients with urgent needs are protected from waits, queues and backlogs” says Chris Simpson, cardiologist and incoming Canadian Medical Association President. However, evidence suggests that this assumption may not always hold true.
New approaches in acute care surgery
The past decade has seen a movement across some larger Canadian hospitals to improve access to surgical services for patients with urgent surgical conditions. This has been in part motivated by some evidence and concerns from surgeons and hospital administrators that these patients are waiting too long.
Avery Nathens, Chief of Surgery at Sunnybrook Health Sciences Centre, says these programs are driven by the “need to build emergencies into the routine.”
As of 2009, there were 13 dedicated acute care surgery services across Canada. These dedicated services usually mean that the surgeon on call has no other elective cases booked, and can focus on urgent patients. Often, but not always, hospitals with these services have dedicated operating room blocks for urgent procedures so that patients are not left waiting. “Why act as though an emergency is unexpected?” asks Nathens. “Depending on the surgical specialty, over a third of all surgical cases are urgent – why not plan adequately for emergency surgical care?”
Paula Doering, Vice President of Clinical Programs at The Ottawa Hospital was motivated to develop the hospital’s acute care surgery program in response to elective surgeries being cancelled to accommodate urgent cases. She says it was “not fair to patients and surgeons who were getting cancelled.”
Sudhir Sundaresan, Chief of Surgery at the Ottawa Hospital notes that dedicating operating rooms to urgent cases “seemed counter-intuitive” as they were not being fully utilized. However, the costs of maintaining operating room space were offset by the reduction in cancellations for elective surgeries, and fewer patients waiting for surgery taking up emergency department beds. “There wasn’t a patient in the room every minute of the day, which helped to build in capacity and flexibility to meet the needs of urgent cases”, he said.
Emergency department overcrowding and concerns that patients are waiting too long for surgical consults in the emergency department is another motivator for acute care surgery programs. Sunnybrook developed an Acute Care Emergency Surgery Service (ACCESS) program with a dedicated surgeon and operating room for acute care surgery patients. A review of the data after ACCESS was implemented found that it reduced the time it took for surgeons to consult and book urgent patients for surgery, as well as improved emergency department overcrowding.
Fred Brenneman, a surgeon at Sunnybrook who participated in the development of ACCESS, notes that an acute care surgery program may not applicable for all hospitals, and in particular small hospitals. However, he says “there probably could, and should, be more effort into measuring these waits and patient flow.”
We can’t manage what we can’t measure
Stewart Hamilton, former chair of the surgery department at the University of Alberta hospital in Edmonton explains that the “whole picture” is not being measured for urgent surgery patients. He says that in Alberta wait times are collected for emergency department waits, as well as waits once a patient has been booked into an operating room, but that this information is not put together to be able to measure the full wait for urgent surgery patients.
Doering describes trying to measure waits for urgent surgeries as “a nightmare” with multiple, disconnected data sources from different parts of the hospital.
The public reporting and measurement of wait times for elective surgeries, along with significant government funding to increase the number of surgeries, has helped to reduce waits for some surgical procedures across Ontario. However, Nathens suggests that in this environment where elective surgery wait times are being counted and measured, surgeons feel pressure to meet government-set targets. He says “everyone is so focused on making their targets that there is the potential for urgent surgical patients to be left behind.”

The comments section is closed.
The wait times in Alberta are ludicrous. I have a referral from the er department for gallbladder removal. finally heard from surgeon and its a 9 Month wait just for a consult and they consider that to be emergency referral. Was told to get my doctor to write a letter stating my case as urgent which i have done and it didnt help at all. how much more urgent can it get from a emergency room referral? This is not acceptable. I cant eat anything.. most days i cant even keep water down. Er doc advised to eat a “bland” menu. I cant sleep as im in severe pain all day and all night. what has to happen for people to get the medical care that is so urgently required?
Why won’t anyone on Surgical team call me?
I was schudeled with a Surgical fat last week and today I have been told they have nothing on me at Surgical booking
i’ve been waiting two months for a reschedule for herniated disc surgery and have no idea what to expect… cannot reach the surgeon, no calls returned from the doctors office, missed a call last week from the doctors’ 407 prefix while i was seeing my GP and cannot reach anyone involved in my case… this is not an elective surgery and it’s been eight months since the MRI and the diagnosis and no clue how to comprehend this process… now i fear due to the missed call that i’ve been bumped to the bottom of the waiting list or removed altogether but how would i know? whom should i call?
I am I the same boat. Floating around in pain that gets worse every day. The depression is worse…. (Not really). I can’t work. I have no money left and none coming in. I am on an emergency list for double herniated disc replacement. It has been 6 weeks since my first re-schedule. The receptionist called ” get ready for surgery in 4 days!!” Then nothing. No phone call. The office was shut down for 2 weeks. Then the surgeon was away for 2 weeks. Now I have waited for another 2 weeks and NOTHING. I am frustrated. My GP is useless. She is barely able to help me. I had to fight just to get X-rays and mri’s. I am so exhausted. This has been a 9 month ordeal so far. I have lost the jobs I had and any support from friends and family (extended family). I offered to go to another province but was told I would not receive any care once I got back. What the hell are you supposed to do??
i was hit in my driveway by my neighbor and my husbnd rushed me to Mt, Sinai emergency.My femur is broken and I need a metal plate in my knee After 11 hours I was admitted to the hospital.I was moved from emergency to a rehab ward where I have been shelved each day, denied food and drink til 7pm and bumped to the next day. It has been FOUR 24 hour days going into the 5 th.What are my options for getting scheduled for an operation? Is there a system for transfer if after this length of time \surgery cannot be scheduled? HELP
Aren’t these specal times, i’m glad to be alive in these times.
https://www.gynecomastia.org/scientific-articles
wife had shoulder surgery 0ne year ago which didn’t work and know on another waiting list to have it fixed
Patient groups realized in 2004 when the measuring of wait times for Hip and Knee surgery began that it would impact wait times for other surgeries that are not being measured. I am baffled that “experts” couldn’t have predicted this outcome. In addition to waiting too long for emergency surgeries wait times for foot, hand, elbow and shoulder surgeries have grown. Another reason to include the patient perspective in health policy development!
There are some hospitals in the U.S. which will not allow for “conservative management” protocols of urgent conditions — even if such management helps some patients — because it can be a slippery slope.
If you are allowed to delay emergency surgery, and there is administrative pressure to manage the patient load, will the decision to delay really be made in the patient’s best interests?
For more discussion on this article, see Every Patient Matters on Facebook: https://www.facebook.com/impatient4change/posts/547734561959530
Great article. I found it interesting that you admitted, as is often the case, that the surgeon booked call on his OR day. Does this qualify as being available on call?
Shawn
http://www.shawnwhatley.com
Why not plan for urgent surgical care? – ask some. Because operating rooms dedicated to urgent cases will be underutilized – reply some others. That’s true. When demand varies, the only way to avoid waits is to maintain surplus capacity. The debate therefore shifts to the issue of how much surplus capacity is achievable. Well, when capacity is fixed by the budget, the surplus capacity for urgent procedures could only come from reducing capacity for planned procedures. However, current evidence is mostly insufficient to justify the changes in hospital care that would be required to prioritize access to some procedures at expense of delaying the others. For example, Canada’s health ministers adopted 48 hours after admission as a benchmark for the provision of hip fracture surgery. However, investigators are yet to identify groups of patients who will benefit from accelerating their surgery through the 48-hour commitment.
Surprisingly, we could easily test whether postoperative complications and in-hospital deaths were more frequent among patients who received hip fracture surgery beyond 48 hours after admission. The delivery of hip fracture care in hospitals across the country creates a natural experiment for studying health outcomes of surgical delays, because patients had to wait for various times before undergoing the procedure. And there is a pan-Canadian group that collects data on all hospitalizations with the date and time of admission and the date and time of procedure, enter the Canadian Institute for Health Information. In a recent submission for a grant to CIHR, a group of surgeons and health services researchers argued that wide variation in time to surgery and case mix across Canadian surgical services offer sufficient statistical power to detect true differences in health outcomes among patients with various wait times. The proposed pan-Canadian collaboration provides the opportunity to describe the results of surgery in hospitals across the entire country according to a standardized methodology for defining index admission and care episodes. The evidence generated by our research will inform decision-makers involved in allocating appropriate resources to minimize the adverse effects of delays in providing hip fracture surgery.
Nice article. %featured%Another example of shortsighted decision-making without consideration of unintended consequences. In most centres, unscheduled events (admissions, surgeries, ER visits) follow predictable patterns, so it should not be difficult to build estimates of unscheduled demand into capacity plans. Variation in demand for health care services is unavoidable (scheduled surgeries are a major source of variation), and simple queueing theory tells us that having buffer capacity makes sense. %featured%Hospital administrators and funders often miss the fact that running a service at close to full occupancy will necessarily result in delays for care, especially when care processes are highly variable and inefficient (which they often are).
Wait times create a heavy burden on Canadian patients, caregivers, employers and the economy through worsening of medical conditions, lost productivity and revenues, and other effects. Our health care system may be set up to make us wait, but innovative practices and new approaches can and are making a difference in reducing wait times within the system. One such example in the surgical setting is the Saskatchewan Surgical Initiative (SKSI), which is successfully bridging the gap in identifying and measuring surgical wait lists, then employing initiatives such as pooled referrals to speed up the time to surgery. The Health Council of Canada’s latest video series “Innovations in Reducing Wait Times” looks at this as well as other innovative practices across Canada working to reduce wait times: http://www.healthcouncilcanada.ca/waittimes
In January 2013 I reported as instructed a worsening symptom in my back problems to my gp who referred me back to my orthopedic surgeon. The process of seeing the surgeon, getting the required MRI, getting the follow up appointment and then being placed on the wait list took until December 29/2013. I was told I will be waiting 7-9 months for my spinal stenosis and herniated disk surgery on top of that. I am barely able to walk and must use canes when I do and my condition deteriorated daily, I live in 24/7 pain as there is no medication for nerve pain that my body will tolerate any more. I also have severe muscle spasms from this condition every night so I get very little sleep due to be awakened every hour or so. I no longer can go to church, travel or shop except for the groceries I have to have. I rarely see friends or family as it is just too difficult to socialize when you are in extreme pain all the time. My physical shape is getting worse as I am unable to exercise due to the pain in my feet and legs. So, please do not tell me that wait times in Saskatchewan have improved. I have had the same surgeon since 2008 and he is very familiar with the terrible shape I am in but there is nothing he can do to speed up the process. It is all very well to talk about pooled referrals and being given a different surgeon but we can all check the ratings on surgeons and do not want one with a bad reputation when we are faced with life altering surgery. I feel for the health care professionals who have to work in this broken system-they are victims of excessive bureaucracy just as we patients are-except they will not have to face the possibility of severe health consequences due to the wait system. Referring back to the information I gave above I will have been waiting almost two years for my needed surgery.Wait list times should be calculated when the process starts; not when the referral to the wait list is made.