Greg Price died at the age of 31. His death may have been preventable had he been diagnosed and treated earlier for testicular cancer. He was left alone to navigate the health system and follow up on referrals, while experiencing major delays and the absence of communication and information.
His journey through the health system, and untimely death, were the focus of a December 2013 Health Quality Council of Alberta (HQCA) study. The study highlights the need to ensure that test results and referrals are better communicated in Alberta to patients, and between health care providers. Alberta’s Minister of Health Fred Horne called Greg’s story an “an indictment of the health system” noting that “the system clearly failed this patient.”
Greg’s journey: falling through the cracks of the health system
Dave Price, Greg’s father, describes his son as selfless, saying that this may have put Greg at a disadvantage as a patient. Price says he often wonders if “had he been more selfish, rather than selfless, more aggressive than respectful, maybe things would have been different.”
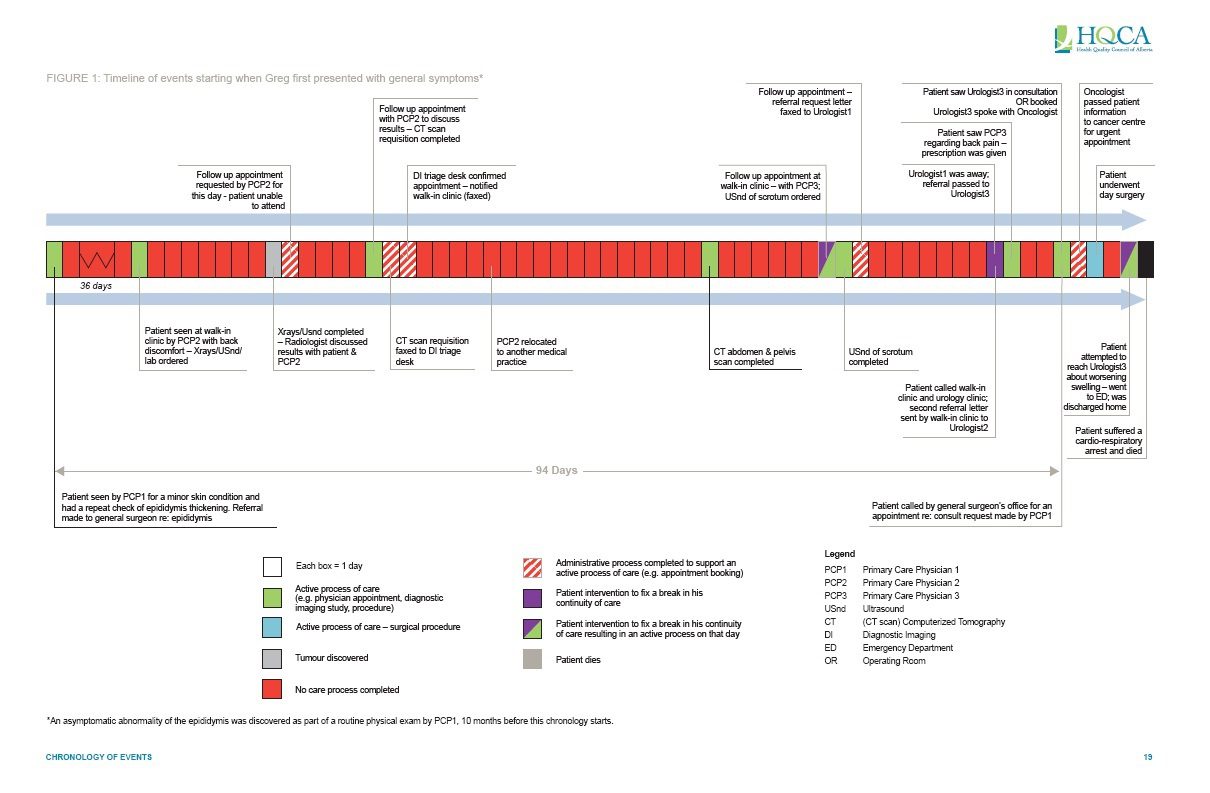
Greg’s difficult journey through the health system is detailed extensively in the HQCA study and on his family’s website. Click here to see a full chronology. The following section provides an overview of the last months of his life.
{kind=link}
During a routine physical exam at a primary care clinic, it was identified that there was thickening of a tube of Greg’s testicles. The physician made a note that Greg should return for an assessment if he experienced any changes, or follow up in a years’ time.
At his next encounter, nearly a year after that first visit, Greg visited the same primary care clinic, at which point it was decided that he should be referred to a general surgeon for further assessment. However, it took 3 months for this appointment to be scheduled, with no feedback to the referring physician or Greg on when he should expect to have an appointment, or how long it would take.
In the meantime Greg like 1 in 4 Canadians each year, visited a nearby walk-in clinic because of back pain. The physician he saw there ordered a number of tests which detected a large mass in his abdomen. Greg and this physician discussed a possible cancer diagnosis. Follow up tests, including an abdominal CT scan, marked as urgent, were ordered.
It took three weeks for the CT scan appointment to be completed. During this period, the physician who Greg saw at the walk in clinic left that practice, and Greg received no information about the CT scan results.
Clearly concerned, Greg phoned the walk-in clinic and was told the physician who ordered the tests no longer worked there. Greg was seen by another physician at the walk-in clinic who reviewed the tests, and sent a referral to a urologist for surgical consultation.
During this time Greg experienced increased back pain and high blood pressure, presumably caused by the mass in his abdomen. He was in pain and was regularly checking his own rising blood pressure at drug store blood pressure machines, becoming increasingly worried.
A week after the referral was made to the urologist, Greg had not heard back about an appointment so he phoned the walk-in clinic, which suggested he call the urologists’ office himself. When he did, there was a recorded message stating that the urologist was away for an extended period of time. There was no one to speak to at this office, and no way to leave a message. Greg relayed this information back to the walk-in clinic, who booked him in for a consultation with another urologist for a few days later.
At the urologist appointment, and a day before surgery, an urgent referral was made to an oncologist.
Within a few days, Greg had surgery to remove the testicle which was found to contain cancer, and upon returning home from this day surgery experienced swelling of his legs. Even though it was a Friday, the office of the urologist who performed the surgery was closed in advance of the Victoria Day long weekend, and Greg had no follow up instructions for what to do in the case of complications other than to go to an emergency department.
Greg’s family took him to the emergency department. He was sent home after being assessed by a physician and it was confirmed that he would be seen by an oncologist later that week. In the early morning hours following emergency department discharge, Greg collapsed at home due to a blood clot, a common post-surgical complication, and could not be resuscitated.
Making sense of Greg’s death
Greg’s untimely death was a shock to his family, friends and community. His funeral took place at a packed hall in his hometown of Acme, Alberta with over 600 people present. One characteristic comment across the eulogies was Greg’s tenacity.
His father proudly says “he excelled through an incredible level of commitment and focus.” Greg was trained as an engineer, worked as a pilot and had founded a company. He was also an accomplished athlete – playing baseball and basketball for the province of Alberta while in high school, and continuing to play recreationally until a few weeks before his passing.
This tenacity, which characterized Greg’s life, has been taken on by his family to identify and suggest health care system improvements that could have prevented his death.
The Health Quality Council of Alberta (HQCA) learned about Greg, and found that the major gaps in his care reflected survey responses from Albertans rating their patient experiences. Less than 50% of Albertans rated the coordination of their care by health care professionals as excellent in 2012, a figure unchanged since 2003. This is in spite of continuity of care being a major focus of Alberta’s Five Year Health Action plan, initiated in 2010.
The HQCA study includes in its introduction how Greg Price’s experience not only “reveals opportunities to improve Alberta’s health care system” but also underscores “that breakdowns in the system are not merely problems on paper – they affect real people.”
The study’s lead author and HQCA medical advisor Ward Flemons notes that the study doesn’t aim to lay blame on individual physicians, but rather on the system.
“While there is a tension between individual accountability for Greg’s care, and system accountability, if it was just about a few physicians there wouldn’t have been a need to do the study” Flemons says.
Trevor Theman, Registrar of the College of Physicians & Surgeons of Alberta (CPSA) says that there are various levels at which Greg Price’s story can be addressed. He notes that while the study focused on system level issues, when it is found that individual professional obligations and standards are not followed, the CPSA has the capacity to investigate and discipline physicians and “address the individual practice concerns around physicians’ practices” from whom Greg sought care.
A continuous, collaborative and patient centred health system: recommendations
The HQCA study included 13 recommendations, many of which focus on creating what Dave Price describes as a “vision for the health care system” –continuous, collaborative and coordinated patient centred care. This article focuses on the recommendations specific to continuity of care.
eReferrals
Greg experienced major gaps in communication. Recommendations highlight that better systems are needed to ensure that referrals, requests for appointments and urgent diagnostic test requests are dealt with in a timely manner.
Ed Brown, Chief Executive Officer of the Ontario Telemedicine Network says that current referral practices of “just sending a fax and having wishful thinking” are outmoded.
While Alberta has a province-wide electronic health record system, Netcare, not all physician practices have it in place. Netcare is designed to allow authorized users (such as clinicians) to see all prescription, lab results, diagnostic images and hospital discharge summaries for a patient in one place. The study recommends further investment in an eReferral system connected to Netcare which would standardize how referrals are sent, received and completed for all involved clinicians and patients.
This system would standardize the referral process for appointments and diagnostic scans by tracking the process steps from the time a referral is made, completed and results are available, and make this information viewable to patients and physicians.
Prioritizing urgent cases & establishing time commitments for time-sensitive conditions
While the possibility of a cancer had been discussed between Greg and the walk-in clinic physician, there were a number of delays in Greg receiving diagnostic tests and appointments with specialists.
The study suggests that “time-sensitive health conditions” receive priority by radiologists who review diagnostic test results, and radiologists should be allowed to order further diagnostic tests, as appropriate, and to directly refer patients to a specialist, rather than having to go back to the ordering physician, and then wait again for a referral. These referrals would include notification to the ordering physician, and would presumably cut down on waiting times between diagnostic tests and appointments.
Recommendations call on the Alberta Society of Radiologists, Alberta Health Services and the Alberta College of Physicians and Surgeons (CPSA) to develop policies and procedures to support these changes, and identify circumstances that would be considered ‘time sensitive’. Theman highlights that this could be a challenge to implement, saying defining time sensitive is “problematic and will have some push back as it is difficult to legislate and define clinical judgment.”
Physician commitment to patients: availability, after hours access & most responsible physician
Greg found himself without a constant physician contact, having seen multiple physicians at the primary care and walk in clinics, and waiting for referrals to multiple specialists. There was no one person who knew the full picture or was accountable for managing his care.
The study recommends that Alberta Health Services and CPSA revise bylaws to ensure that in cases where patients have a time sensitive health care condition, a ‘most responsible physician’ is identified and known amongst all physicians who provide care to this individual. The most responsible physician is accountable, and available to coordinate care, and respond to urgent requests for patients with time sensitive health conditions, or who have recently undergone treatment.
In addition to identifying a ‘most responsible physician’, recommendations identify the need for better monitoring and compliance with CPSA ‘After Hours Access to Care Standard’. This requires physicians to make specific arrangements for appropriate coverage when they are not available, such as providing patients with contact information for a physician on call.
The standard notes that it is not acceptable to just have a recorded message telling patients with an urgent concern to proceed to the nearest emergency department, and that practices need to have formal agreements in place with the organizations to whom they are directing patients after hours. This was highlighted in Greg’s case because he had just undergone a surgical procedure but was unable to contact the surgeon when he experienced complications.
A CPSA survey found that about 20% of Alberta physicians were not aware of this standard. A Canadian Medical Association Journal editorial published this week highlights that the issue of practice coverage is a challenging, but an essential professional obligation for physicians across Canada.
Theman said in a recent letter to CPSA members that “it’s not good enough to be ignorant of the Standards and it’s not acceptable not to have in place a system for after hours coverage of one’s practice”
Will the HQCA study improve continuity of care for Albertans?
In the weeks following the study’s release Alberta Health Services, CPSA and Alberta Medical Association issued statements in support of the recommendations. These organizations all committed to reviewing recommendations, and working towards their implementation.
Study recommendations, in particular around eReferral systems, require significant investments of dollars, and major cultural shifts to how physicians communicate and practice.
Ward Flemons believes however that “there is hope that this isn’t pie in the sky thinking and that there is the ability to do it, though it requires commitment and vision.”
Theman agrees, saying that “the recommendations related to physician practice have a good prospect of change” and that there is a willingness among physicians to improve systems of communication and practice.” He also highlights a sentiment among some physicians of the risk that “the public could lose trust in the profession’s ability to self-regulate unless many of the recommendations are addressed.”
Greg’s family has also been acknowledged as a driving force for improvement. Flemons says “while everyone wants change, they are truly committed and will do their best to hold people accountable.”

The comments section is closed.
Absolutely agree with HQCA study recommendations. Issues with referrals is well know. The issue is not a complex one. Government can simply decree to its doctors that all referral information must be communicated and accepted by the patient. Define data requirements, timeliness, responsibilities and methods of communication. This is simple business analysis and some computer programming. But governments have no motivation to fix the problems associated with referrals or it would things would have been fixed by now. Government benefits by delaying referrals, not hiring enough doctors and hiding behind what is really going on with our system. Unfortunately government agendas are in conflict with patient needs and doctor remuneration. This needs to be fixed and policy must align with Freedom and Information and Protection of Privacy legislation which says that the patient is responsible for their information and they are the ultimate owner of their personal data.
Until patients are given the information they need and the tools to manage their own health care nothing will change.
Patients don’t know that they have the right to know if an appointment has been booked, if a report has been delivered etc And if these things don’t happen patients don’t know what they’re supposed to do, or who to contact. We’re lambs to the slaughter.
Depending on overworked ever changing ‘family doctors’ to provide patients with this level of care is asking too much. Fold in the arrogant paternalistic attitude still prevalent in health care providers in Canada and you have a recipe for disaster.
EMPOWER THE PATIENT WITH KNOWLEDGE.
When Canadians start demanding better service levels only then will the medical profession smarten up.
There are systemic flaws in Canada’s health care system that need be addressed before cases like that of Greg Price become more the norm than the exception. Canada’s two tired health care means the wealthy fly south rather than wait the months for elective surgery that if left unattended can become life threatening.
Not in my lifetime
Such a complex issue.
One thing I do know: our healthcare system in Ontario is fragmented and segmented by differing funding bodies and government pockets. How can we achieve a truly integrated healthcare system when there is diversity in funding?
Add to that the vested interest many healthcare providers have in maintaining their empires of control and the goal is further obfuscated.
The patient (and taxpayer) is the ultimate loser in this perpetual tug-of-war.
This story sums up so much of what is wrong with the current system. While it is true that the system has failed this man, rather than any one individual, I wonder if after-hours and out-of-office accountability are perhaps not receiving sufficient attention in our medical training. So much emphasis has been placed on communication skills, interdisciplinary care, and all the other CanMeds roles that the 24-hour, 7-days a week sense of commitment to patients may now be relatively de-emphasized. We often hear stories about a previous generation of physicians, who made house calls, went to see their outpatients when they became hospitalised, and could be reached, personally, even after hours. This has been lost.
While bringing this sort of culture back raises concerns of time pressures and lack of sustainability for the large number of patients in a practice, it makes me wonder how it was done in the past. Could a new system of fee codes used to pay for more support staff (nurses, extended hours admin support) draw physicians toward a more accessible practice model?
The paradox is that these models of care are much more expensive .
Welcome to the rabbit hole, William.
The rallying cry of the university medical management programs in the 90’s was to ‘break the medical model’. They don’t ‘get’ us and what you don’t understand you can’t manage. Thus the proliferation of non-evidenced based team-centered models and their multiplicity of unintended consequences like two-tiering, increased expense, compromised patient care and follow-up, and a burgeoning administration growing and metastasizing like a malignancy.
When the system fails as it so obviously did in this case the response is the blame the docs and suggest yet another layer of bureaucracy.
You took the words out of my mouth!
I am a new physician in a non-primary-care specialty, and I was loathe to drink the Kool-Aid of the “team centered” model of care that so permeated through the medical school curriculum.
The doctor is not the pointman, the doctor is but a member of the “team”. Everyone is important, because its a “team”. Bla bla bla.
The truth is with the advent and pushing of the team-based concept of health care, which I believe has political motivations to weaken physician autonomy and empower ancillary staff with the hopes of lowering total health care cost, the patient-centered/doctor-patient relationship model of health care that we have taken for granted has been damaged. Look no further than the unfortunate story above.
Fee-for-service also ensures that the patient’s care is not diluted. If the doctor is paid by the public purse, which was paid by the patient, then that doctor has no administrative suit to answer to. I’ve seen physicians who work as “employees” and boy, they are walking on eggshells and providing substandard care in the name of keeping “quality metrics” high and costs low so their nurse-manager/MBA “boss” won’t fire them. Advocacy FAIL.
It’s time doctors take back medicine. For the patient.
This is truly a sad and unfortunate case. No doubt we will see more of this because the proliferation of the so-called team concept of medical care. Prior to the promulgation of these groups the patient would’ve had a relationship with his family doctor/general practitioner. That relationship is a very human and intense relationship that is nurtured over the lifetime of the patient. There is no doubt in my mind that with the patient focused nature of the doctor-patient relationship that there would have been significantly better follow-up by the family doctor.
The new concept of putting doctors in teams dilutes patient care and dilutes responsibility. In fact,the very nature of these teams makes the medical care institution-centered and not patient centered. Even the method of compensation which is based on capitation rather than fee-for-service encourages poor follow-up and if anything leads to a dereliction of care. All of these alternative care systems have been brought in in the absence of significant evidence that shows improved outcomes. The fee-for-service model, which to paraphrase Churchill is the worst system except for all the rest, implies a direct relationship between patient and physician. I do believe with time and with the proliferation of capitated team base medical care that we will see more of the cases described in this article.
Physicians’ insistence on jealously guarding their autonomy and independence is at the root of this issue. If physicians were required to put systems in place, like EHR access in their offices, electronic referral systems which also allowed the referring practitioner to select the shortest wait time for a consultation, reasonable office clerical/admin staffing to ensure timely feedback when a specialist is unavailable, and RN nurse-navigators to help track patients throughout the system and ensure they do not fall through cracks like this unfortunate young man, these things might not happen.
Hi Gerry, it is our autonomy in Independence that allows us to be free from political interference and allows us to advocate for our patients. The kind of political interference that leads to the chaos and confusion that is currently characteristic of the systems of healthcare delivery produced by government. These systems are not evidence-based unlike the empirical based medical model which dates back to 17th century England.
Indeed, the main reason this patient came to harm his because he went to a primary care clinic where his health care was depersonalized. Instead of being part of a doctor-patient relationship he was part of a clinic patient relationship. This causes diffusion of care with the end result that no one person takes responsibility for the patient.
At great personal expense most of the doctors in Ontario have EHR systems in place and that has been the case for several years now. In our province to government has spent $1 billion trying to make an information Highway so that we can communicate with one another and it has totally wasted this money and failed in Its attempt to allow healthcare practitioners to talk with one another.
RN nurse navigators have never been shown to improve healthcare or accelerate healthcare. It is just adding another layer of administration to an already over-administered system.
The real responsibility has to lie with the family doctor in his commitment to care for the patient. This always worked before but with the onset of family healthcare teams we are beginning to see this system disintegrate. I expect many more cases like the one described in this article as patient’s are shuffled off into and overburdened system with institution and administrative based care. Reinvigorating the medical model will obtain patient centered care immediately. In that system the patient knows who is taking care of him, who to go to if they have concerns and who is ultimately responsible to them for their healthcare.
Who is accountable for ensuring these recommendations are implemented? Whose responsibility is it to teach patients that their silence and trust in the system may kill them?
I%featured% think it might be important to clarify that the concept of eReferral is not futuristic thinking – it is scheduled to go live in Alberta in a week or two.%featured% The project team at Alberta Health Services have been working hard on this concept for quite awhile. More info at http://aacm.ca/pdf/2013-conference/Information-Kit.pdf. The challenge is that it is configured as a ‘limited production roll out’ involving 3 clinical issues (breast cancer, lung cancer, hip& knee surgery) in the province. It is, in the minds of the HQCA the best ‘system-based’ solution for mitigating the risk to patients’ continuity of care – but it will only really do that if it is expanded to include referral management for all conditions and when all referring providers as well as those who provide these types of services sign on to use it. The report calls for additional support to expand this concept to the point that it is the way almost all referral management is done in the province. The report also recommends to make a patient’s referral process (i.e. where they are at in the complex process of getting access to specialized healthcare services) visible to them through NetCare (the provincial EHR) by creating a patient portal.
All of this process implementation and other such MBA buzzword drivel is meaningless.
The fact of the matter is that primary care is undervalued, specialist care is fairly valued, and thus there are no physicians to advocate for the patient.
If Mr. Price was in the care of one primary physician who knew him, that physician would certainly be on the phone getting things in order.
But doing this kind of physician work is not profitable; in fact it is often cost-prohibitive. Offices that have this model of care can go under very easily.
I also fear that we, as physicians, are being brainwashed into withholding proper care based on system cost. The ER physician in the story probably didn’t order a leg doppler (it sounds like Mr. Price was done in by a Pulmonary Embolism), and I wonder if cost-containment factored into this decision. This is all assumption.
Our system fails patients. I am saddened. Back to the walk-in clinic.
%featured%Lack of systems view, which combined by the lack of accountability of individual physicians who are each experts in their own small field of science has led to loss of “care” in the health care system. We no longer have a health-care-system, it’s about disease, we have taken the care out and it is not a system.%featured% Privatize some of the system.
%featured%Implemented yes…enforcement, accountability and associated metrics will be the next challenges and need to be delineated (and funded) early in the process.%featured%
Metrics are only is good as what they measure. Often the government measures metrics which have nothing to do with outcome. For example in our emergency department length of stay is become the holy grail and of course is more of a measurement for political outcome as opposed to medical outcome.
I think the real problem bureaucrats have no idea what doctors do and how we do it And how to measure success.
Clearly the case in question was complete failure of the system, it is the outcome of the government implementing changes to medical care in the absence of any empiric evidence that those changes will work. Since they are guided by a political system that measures outcomes in 4 year aliquots this is only going to get worse in the short-term.
Greg’s outcome may thankfully be rare, but his experience is not. I gave a talk recently about early follow-up care post ED discharge for patients with chronic disease (several ICES studies now show it to be an important predictor of long term outcomes including death) and an emerg doc in the audience told of how patients their tertiary emergency department refer for out-patient follow-up to one of their own hospital’s specialty clinic can be refused because they are not complex enough, but this refusal is communicated days after the patient has left the emergency department, creating a major risk the patient will never get follow up from anyone.
%featured%There needs to be better accountability by doctors receiving consults, not just to be available to receive the request but to carry out appropriate prioritization of referrals and see patients in a reasonable delay. At the same time, referring doctors need to be accountable for the consults they send, so as not to be sending inappropriate consults which may clog up the consultant’s schedule%featured%. And how about the ability to call up a specialist just for some informal advice when maybe all that’s needed is to “run something by” the consultant? Are we too terrified of the medico-legal consequences, or does it require a level of trust and familiarity between primary care docs and specialists that’s rare now outside of rural areas? Finally, why don’t we align incentives and measure performance if we see this as being an important issue?