Surveys indicate that as many as 30 per cent of parents are understandably hesitant to vaccinate their young children, further underscoring the need for COVID-19 vaccination education and outreach and emphasizing the importance of updating families as relevant data emerge from vaccine trials and registries.
However, choosing not to get a vaccine is not a risk-free choice; rather, it’s a choice to take a different and more serious risk. The responsible media and the public health community must strive to make this clear to the public. It could be one of the most important health decisions a parent will make.
We should all have to read a recent terrific editorial on pediatric vaccines by Katharine Smart, president of the Canadian Medical Association, last August. This is exactly what has been on our minds for months as responsible parents, teachers and researchers. In her editorial, she wrote: “Some have suggested that ‘children won’t die of COVID-19.’ Mortality is a crude outcome measure in paediatrics. What about disability, medical trauma, impact on families and mental health? … Preventable death and disability are not acceptable consequences. As the denominator of children with COVID increases, so will the adverse outcomes. It’s simple math.”
Furthermore, children with certain underlying chronic medical conditions are at increased risk for severe COVID-19. The Canadian Pediatric Surveillance Program reported that 39 per cent of children admitted because of COVID-19 had at least one underlying comorbidity, most commonly chronic encephalopathy, obesity, asthma, chronic lung disease other than asthma, epilepsy and neurodevelopmental disorders.
Emerging variants of the SARS-CoV-2 virus are of concern. The more transmissible Delta variant and the emergence of the Omicron variant point to the urgent need for vaccine uptake among children younger than age 12. Recent data indicate that the Delta variant can rapidly spread in schools when unvaccinated adults, such as teachers and staff, come into close contact with unvaccinated children. Not enough is known yet about the Omicron variant to know how it will affect us. However, available information shows that the variant has more than 30 mutations on its spike protein – the key used by the virus to unlock and enter our body’s cells – more than double the number carried by Delta. Such a dramatic change has raised concerns and many countries have once again mandated the wearing of face masks in stores and on public transit, launched stricter quarantine and testing measures for travelers and expanded access to booster shots. Says U.S. Centres for Disease Control director Rochelle Walensky: “The recent emergence of the Omicron variant (B.1.1.529) further emphasizes the importance of vaccination and prevention efforts needed to protect against COVID-19.”
Results from South Africa are still preliminary but suggest that hospitalization rates for children infected with Omicron are higher than were seen in previous waves. As more data emerge, researchers will be looking particularly at the effects of Omicron on children. In a nutshell, however, the vaccines continue to offer protection against severe disease and death. In the South African real-world study (based on 211,000 positive COVID-19 cases and 78,000 cases attributed to Omicron), Pfizer vaccination provided 70 per cent protection against severe complications of COVID-19 requiring hospitalization.
According to the CDC, COVID-19 vaccines are expected to offer protection against severe illness, hospitalizations, and deaths from the Omicron variant as well as other variants. Omicron’s rapid spread further emphasizes the importance of vaccinations, boosters, and prevention efforts needed to protect against COVID-19.
As schools reopen after the holiday break, there will be an urgent need to prevent further school outbreaks and continue uninterrupted in-person learning – the most substantial effects of the pandemic on children have been disruptions in educational, physical and social activities rather than direct viral effects. Available research clearly shows how children have experienced significant trauma from the fallout of the pandemic; school and child-care shutdowns have contributed to a marked increase in behavioural health concerns along with learning loss. Minimizing the burden of COVID-19 through increased vaccination is of urgent importance to help keep children in school.
Although there is much more to understand about the role of children in transmitting SARS-CoV-2, one Canadian study has shown that younger children have greater odds of transmitting to household contacts than older kids. As such, by vaccinating our younger children in a timely and important manner, we can help blunt this COVID-19 wave and any others during the cold winter months, a season in which we know respiratory illnesses can spread more easily.
A clinical trial involving more than 2,200 child volunteers aged 5 to 11 has shown that the vaccines are remarkably safe and effective in preventing serious disease, with no severe adverse reactions. More significantly, the results are notable because they demonstrate good antibody responses and 90 per cent efficacy.
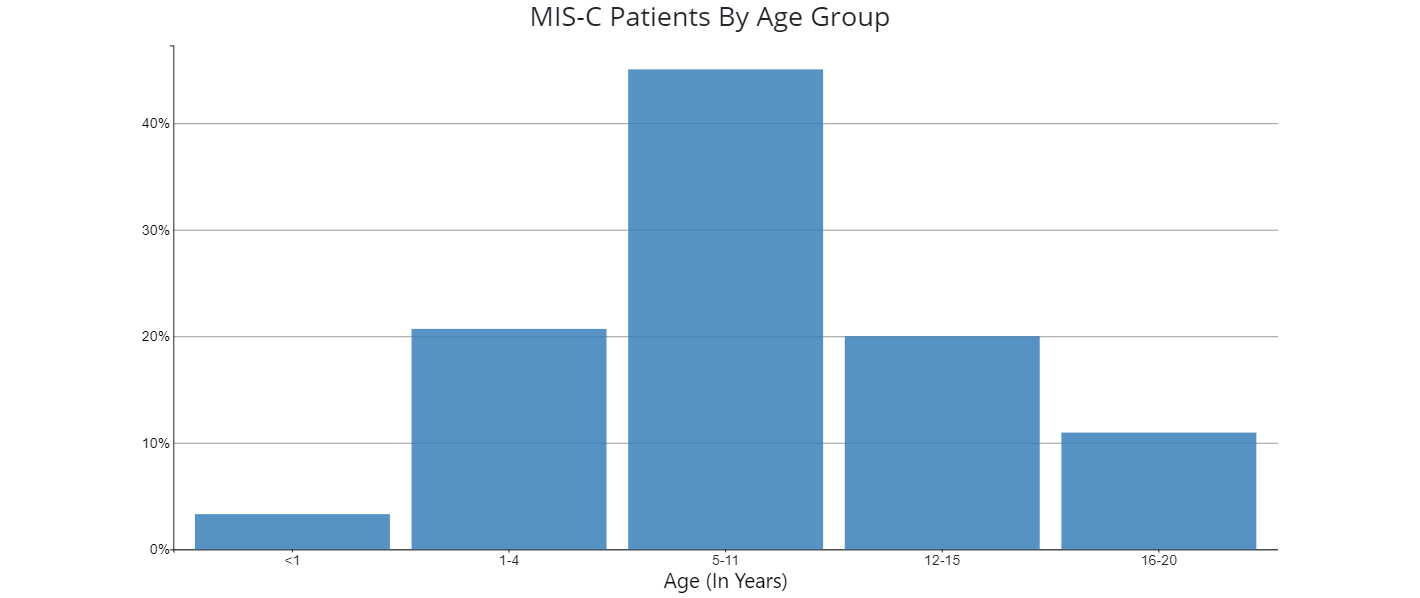
While COVID-19 has typically shown to be mild in children, some have had serious illness. We need to be mindful about Multi-system Inflammatory Syndrome in Children (MIS-C), a condition closely associated with COVID-19. MIS-C causes several parts of the body to become inflamed, including the heart, lungs and eyes. Two in three children afflicted with MIS-C have reported ongoing symptoms more than 60 days after diagnosis. A recent study in the Journal of the American Medical Association estimates that the risk of MIS-C among adolescents is significantly higher among the unvaccinated, clearly showing that COVID-19 mRNA vaccination is associated with a lower incidence of MIS-C in adolescents.
Source: https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance
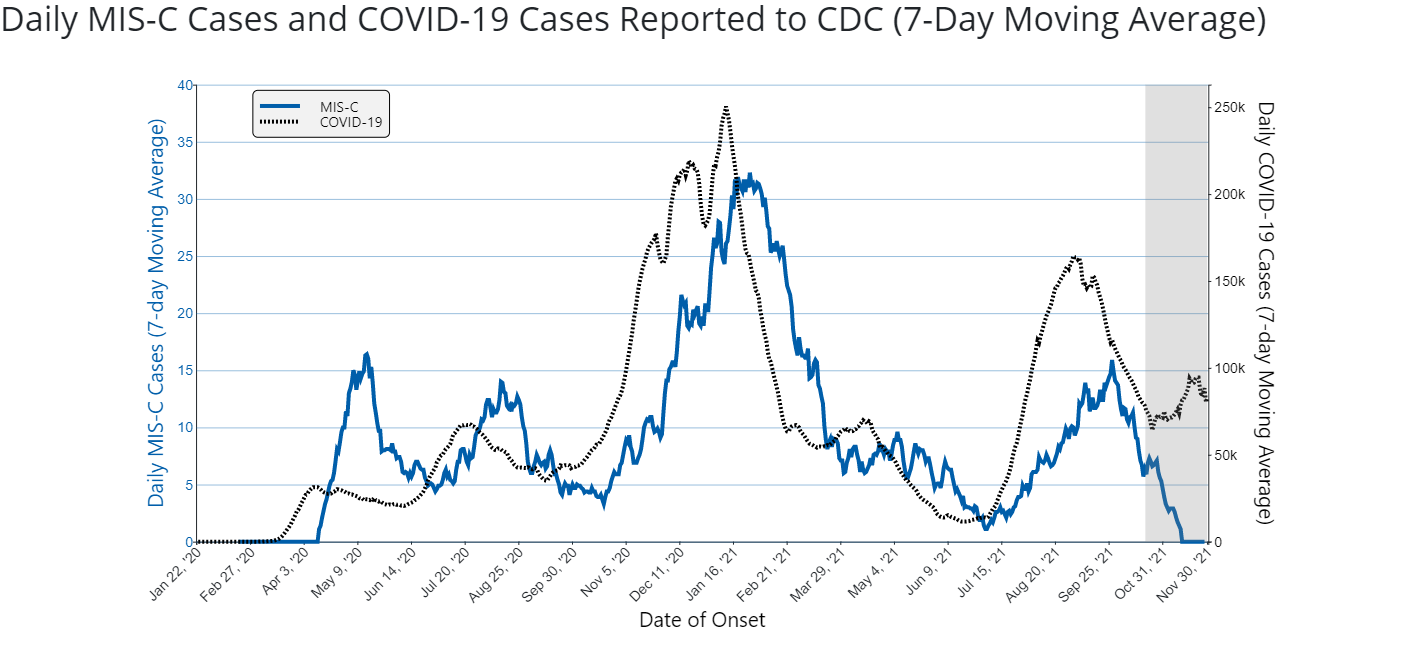
Number of included MIS-C cases: 5,969. The graph shows the 7-day moving average number of COVID-19 cases and MIS-C cases with date of onset between February 19, 2020 and November 22, 2021. The grayed-out area on the right side of the figure represents the most recent 6 weeks of data, for which reporting of MIS-C cases is still incomplete. The actual number of MIS-C cases during this period is likely larger, and these numbers are expected to increase as additional case reports are incorporated. The scale for the Y-axis differs on the left and the right sides of the figure. The left Y-axis marks the number of daily 7-day average MIS-C cases in units of 5 with a scale of 0 to 40; the right Y-axis marks the number of daily 7-day average COVID-19 cases in units of 50,000 with a scale from 0 to 250,000. To protect patient privacy and ensure data stability, data are suppressed when the 7-day moving average is <1. Source: https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance
More than 80 per cent of children aged 12 to 17 in Canada have been fully vaccinated. The preliminary data on vaccine effectiveness in this group is astonishing and should be a strong motivator to inoculate our younger children. A real-world evaluation study demonstrated that two doses of Pfizer-BioNTech vaccine were highly effective in preventing hospitalization among persons aged 12 to 18 (see the table below).
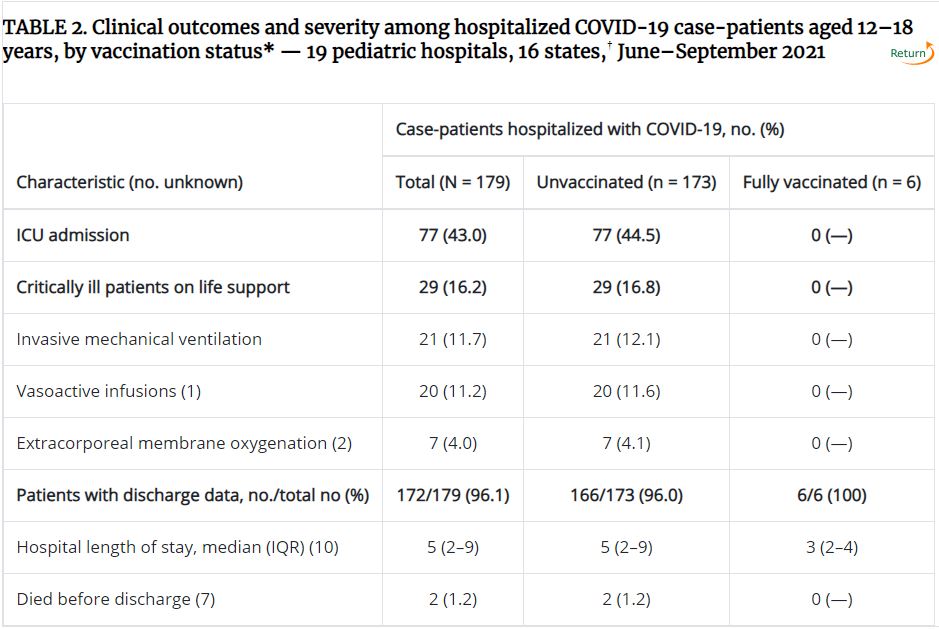

This table has been reproduced with the permission of the CDC. It is from a report originally posted on Oct. 19, 2021, under the title "Effectiveness of Pfizer-BioNTech mRNA Vaccination Against COVID-19 Hospitalization Among Persons Aged 12–18 Years — United States, June–September 2021."
Pediatricians and other health professionals caring for children should be prepared to address the concerns and fears of parents, adolescents and children. Both the Canadian Pediatric Society (CPS) and American Academy of Pediatrics (AAP) advise that informed consent should include discussion about the rare reports of myocarditis and pericarditis following vaccination, what warning signs to watch out for, and the fact that the vaccine’s benefits outweigh the risks.
It is time to provide parents and caregivers – from schools and pediatricians’ offices to clinics and pharmacies – a range of options to vaccinate our younger children. We also urgently need a dialogue with public health decision-makers on logistics to enhance vaccine availability in our communities and organize mobile clinics with respective school boards. Parents and caregivers should be reassured that despite this vaccine’s rapid development, clinical trials and regulatory review have met accepted standards and extensive, ongoing post-marketing surveillance for adverse events is being conducted.
Parents and caregivers of younger children receiving their first dose may be interested in participating in the Canadian National Vaccine Safety Network, which monitors vaccine safety following vaccination. The Canadian Pediatric Society online module, Our best shot at COVID: Overcoming vaccine hesitancy in 2021, provides strategies for dealing with vaccine hesitancy. The National Academies of Sciences, Engineering and Medicine has unveiled actionable guidance to help build confidence in vaccination, especially for parents considering having their children vaccinated.
The pandemic and its profound consequences affirm that every vaccinated individual counts. Since approximately one-third of confirmed cases in minors have been asymptomatic, creating opportunities for them to spread the virus unknowingly, reduction of asymptomatic transmission is essential to slowing the spread of the virus. Having a highly vaccinated population, including children, creates wider freedom to return to the ordinary activities we value.
Countries will need highly protected populations for as long as COVID-19 exists, likely for years if not decades. Vaccinating all children against SARS-CoV-2 could be among the most impactful public health efforts Canada has seen in decades.

The comments section is closed.
Thank you for this great article. Do you have thoughts on opening up vaccine eligibility to kids born in 2017?
At this time, only the Pfizer-BioNTech COVID-19 vaccine is authorized and recommended for children and adolescents aged 5-12. COVID-19 vaccines currently approved or authorized by Health Canada/ National Advisory Committee on Immunization are effective in preventing serious outcomes of COVID-19, including severe disease, hospitalization, and death. Children younger than age 5 years are not eligible to receive the Pfizer-BioNTech COVID-19 Vaccine at this time unless part of a clinical trial. Efforts to maximize the proportion of people in Canada who are fully vaccinated against COVID-19 remain critical to ending the COVID-19 pandemic (this includes Children younger than age 5 years of age). As coronavirus cases in children surge again due to the Omicron variant, vaccine approval for kids under 5 can’t come soon enough for many parents and caregivers. Many had hoped the New Year might bring a vaccine for young children. But it looks likely that the youngest children won’t get protection from Covid-19 until well into 2022 as Pfizer announced last week that it was amending the clinical trial of its vaccine in children 6 months to 5 years old. According to the company sources, two doses didn’t elicit the same kind of robust immune response in 2- to 5-year-olds as with adults. A third dose will be added to the trials for children under 6 and the clinical trial data is expected in early spring. Good news is that Moderna also has an ongoing Covid-19 vaccine trial for kids 6 months to 5 years and the company forecast that the vaccine for this age group could be available as early as the “first month or two” of 2022.
Efforts to maximize the proportion of people in Canada who are fully vaccinated against COVID-19 remain critical to ending the COVID-19 pandemic (this includes children 0-4 year olds). Furthermore, available Canadian study (based on Ontario data) shows that the chances that these vulnerable children get Covid and will pass it along are high, and so we have to vaccinate them to not only protect them but to protect their families and communities. So, this accumulating evidence further shows that they need to get vaccinated when they become eligible for a number of reasons including their own protection and safety. We also can’t predict which kids are not going to do well with Covid, and we’ve certainly had our share of otherwise normal, healthy children who end up with very serious complications including the Multisystem inflammatory syndrome in children (MIS-C) and also they are vulnerable for potential long term impact of Covid 19 infection “long Covid”.
In most jurisdictions in Canada, almost 80% of the patients who are currently admitted in our hospitals with Covid-19 across the medical system are unvaccinated and 8% of all patients who are hospitalized with Covid-19 are vaccinated. Dissemination of real world data on the effect of COVID-19 vaccination on the trajectory of the pandemic is important to verify that vaccines are working as expected at the population level and might increase public confidence in the vaccination program.
New hospital admissions for children under 11 with confirmed Covid-19 are already shown exceeding 1300 cases and among hospitalized children 146 of them are in the ICU. We already lost 14 children due to Covid 19. For our youngest children, those who are not yet eligible for vaccination, it’s critically important that we surround them with older siblings, parents and caregivers (including daycare workers/teachers) who are vaccinated to provide them maximum protection until safe vaccines are available and approved by Health Canada in the spring 2022.
Great piece, colleagues.
Many thanks.